Department of Biomedical Sciences and Human Oncology, University of Bari "Aldo Moro" Medical School, Polyclinic, Piazza Giulio Cesare, 11, 70124, Bari, Italy.
Clin Exp Med. 2023 Jun;23(2):255-272. doi: 10.1007/s10238-022-00808-1. Epub 2022 Mar 28.
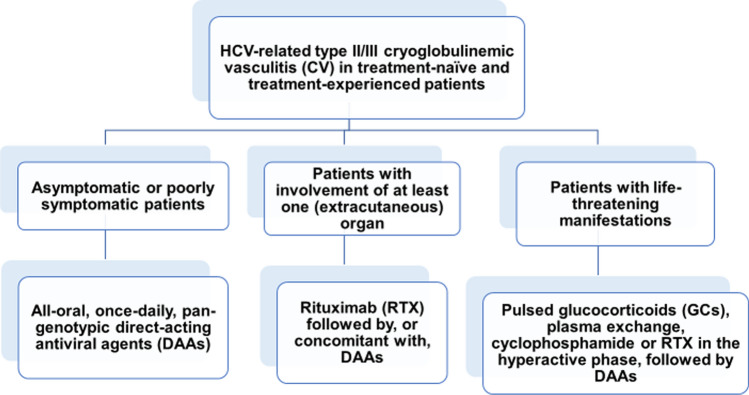
Immunoglobulins that reversibly precipitate at temperatures below 37 °C are called cryoglobulins (CGs). Cryoglobulinemia often manifests as cryoglobulinemic vasculitis (CV), whose symptoms range in severity from purpuric eruptions to life-threatening features. The majority of CV patients are infected with hepatitis C virus (HCV), whereas lymphoproliferative disorders or connective tissue diseases (CTD) are commonly diagnosed among patients with CV of non-infectious origin. In the absence of detectable associated disease, cryoglobulinemia is classified as "essential" (EMC). All HCV-positive CV patients should be given direct-acting antiviral agents (DAAs) that are consistently able to induce a sustained virologic response (SVR). Glucocorticoids (GCs) can mitigate CV-associated vasculitis, but they have no role as maintenance therapy. Cyclophosphamide restrains the hyperactive phase(s) of the disease and the post-apheresis rebound of newly synthesized CGs. Its use has been largely replaced by rituximab (RTX) in patients unresponsive to DAAs, patients progressing to B-cell non-Hodgkin lymphoma (B-NHL) and patients in whom CV persists or reappears after clearance of HCV. Therapeutic apheresis is an emergency treatment for CV patients with hyperviscosity syndrome. HCV-positive CV patients are at an increased risk of developing NHL, but the achievement of SVR can effectively prevent HCV-related NHL or induce the remission of an already established lymphoma, even without chemotherapy. The treatment of patients with IgM or IgG monoclonal cryoglobulins and an underlying immunoproliferative disorder is based on the regimens adopted for patients with the same B-cell malignancies but without circulating CGs. For patients with CTD, GCs plus alkylating agents or RTX are similarly effective as first-line therapy and in the relapse/refractory setting. In patients with EMC, treatment should consist of GCs plus RTX, with the dose of GCs tapered as soon as possible to reduce the risk of infectious complications.
在 37°C 以下温度可逆沉淀的免疫球蛋白称为冷球蛋白 (CGs)。冷球蛋白血症常表现为冷球蛋白血症性血管炎 (CV),其症状从紫癜性皮疹到危及生命的特征不等。大多数 CV 患者感染丙型肝炎病毒 (HCV),而淋巴增生性疾病或结缔组织疾病 (CTD) 在非感染性 CV 患者中更为常见。在没有可检测到的相关疾病的情况下,冷球蛋白血症被归类为“原发性”(EMC)。所有 HCV 阳性 CV 患者均应给予直接作用抗病毒药物 (DAA),这些药物始终能够诱导持续病毒学应答 (SVR)。糖皮质激素 (GCs) 可减轻 CV 相关血管炎,但不能作为维持治疗。环磷酰胺可抑制疾病的高活性期和新合成 CG 在后血浆分离后的反弹。在对 DAA 无反应的患者、进展为 B 细胞非霍奇金淋巴瘤 (B-NHL) 的患者以及在 HCV 清除后持续或再次出现 CV 的患者中,其使用已被利妥昔单抗 (RTX) 大量取代。治疗性血浆分离术是 CV 伴高粘滞血症综合征患者的紧急治疗方法。HCV 阳性 CV 患者患 NHL 的风险增加,但 SVR 的实现可有效预防 HCV 相关 NHL 或诱导已建立的淋巴瘤缓解,即使没有化疗。IgM 或 IgG 单克隆冷球蛋白和潜在免疫增殖性疾病患者的治疗基于为无循环 CGs 的相同 B 细胞恶性肿瘤患者采用的方案。对于 CTD 患者,GCs 加烷化剂或 RTX 作为一线治疗同样有效,在复发/难治性患者中也同样有效。对于 EMC 患者,治疗应包括 GCs 加 RTX,尽快减少 GCs 的剂量以降低感染并发症的风险。