Saeed Sana, Khan Qudsia Umaira
CMH Lahore Medical College & Institute of Dentistry, Lahore, Pakistan.
Discoveries (Craiova). 2021 Sep 30;9(3):e137. doi: 10.15190/d.2021.16. eCollection 2021 Jul-Sep.
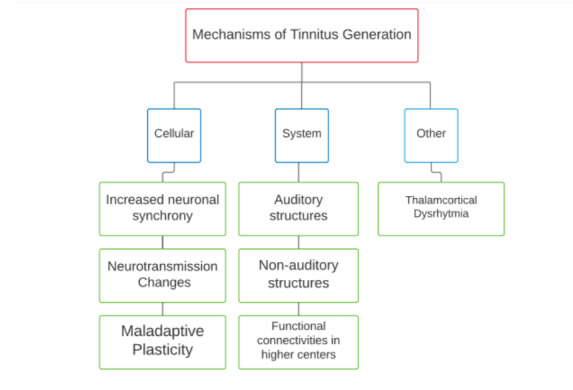
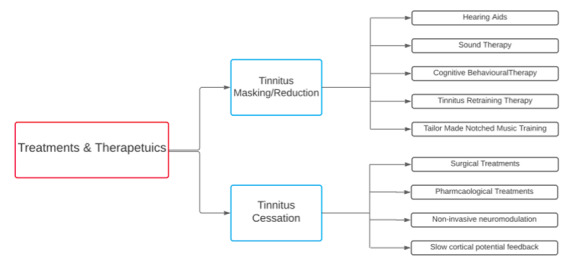
Tinnitus is defined as the ringing, hissing, clicking or roaring sounds an individual consciously perceives in the absence of an external auditory stimulus. Currently, the literature on the mechanism of tinnitus pathology is multifaceted, ranging from tinnitus generation at the cellular level to its perception at the system level. Cellular level mechanisms include increased neuronal synchrony, neurotransmission changes and maladaptive plasticity. At the system level, the role of auditory structures, non-auditory structures, changes in the functional connectivities in higher regions and tinnitus networks have been investigated. The exploration of all these mechanisms creates a holistic view on understanding the changes the pathophysiology of tinnitus undertakes. Although tinnitus percept may start at the level of cochlear nerve deafferentation, the neuronal changes in the central auditory system to the neuronal and connectivity changes in non-auditory regions, such as the limbic system, become cardinal in chronic tinnitus generation. At the present moment, some tinnitus generation mechanisms are well established (e.g., increased neuronal synchrony) whereas other mechanisms have gained more traction recently (e.g., tinnitus networks, tinnitus-distress networks) and therefore, require additional investigation to solidify their role in tinnitus pathology. The treatments and therapeutics designed for tinnitus are numerous, with varied levels of success. They are generally two-fold: some treatments focus on tinnitus cessation (including cochlear implants, deep brain stimulation, transcranial direct current stimulation and transcranial magnetic stimulation) whereas the other set focuses on tinnitus reduction or masking (including hearing aids, sound therapy, cognitive behavioral therapy, tinnitus retraining therapy, and tailor made notched musical training). Tinnitus management has focused on implementing tinnitus masking/reducing therapies more than tinnitus cessation, since cessation treatments are still lacking in streamlined treatment protocols and long-term sustainability and efficacy of the treatment. This review will focus on concisely exploring the current and most relevant tinnitus pathophysiology mechanisms, treatments and therapeutics.
耳鸣被定义为个体在没有外部听觉刺激时自觉感知到的铃声、嘶嘶声、咔嗒声或轰鸣声。目前,关于耳鸣病理机制的文献是多方面的,从细胞水平的耳鸣产生到系统水平的耳鸣感知。细胞水平的机制包括神经元同步性增加、神经传递变化和适应性不良的可塑性。在系统水平上,已经研究了听觉结构、非听觉结构的作用,更高区域功能连接性的变化以及耳鸣网络。对所有这些机制的探索为理解耳鸣病理生理学所经历的变化创造了一个整体的视角。虽然耳鸣感知可能始于耳蜗神经去传入水平,但中枢听觉系统中的神经元变化以及非听觉区域(如边缘系统)中的神经元和连接性变化在慢性耳鸣的产生中变得至关重要。目前,一些耳鸣产生机制已经得到充分确立(例如,神经元同步性增加),而其他机制最近受到了更多关注(例如,耳鸣网络、耳鸣 - 困扰网络),因此,需要进一步研究以巩固它们在耳鸣病理中的作用。针对耳鸣设计的治疗方法众多,成功程度各异。它们通常分为两类:一些治疗方法侧重于耳鸣消除(包括人工耳蜗植入、深部脑刺激、经颅直流电刺激和经颅磁刺激),而另一类则侧重于耳鸣减轻或掩蔽(包括助听器、声音疗法、认知行为疗法、耳鸣再训练疗法和量身定制的滤波音乐训练)。耳鸣管理更多地侧重于实施耳鸣掩蔽/减轻疗法,而不是耳鸣消除,因为消除疗法在简化治疗方案以及治疗方法的长期可持续性和疗效方面仍存在不足。本综述将集中简要探讨当前最相关的耳鸣病理生理机制、治疗方法和疗法。