Medicines Use Research Group, Institute of Pharmaceutical Science, King's College London, London, UK.
Pharmacy Department, Guy's and St. Thomas' NHS Foundation Trust, London, UK.
Age Ageing. 2022 Mar 1;51(3). doi: 10.1093/ageing/afac054.
To determine the association between frailty and medication-related harm requiring healthcare utilisation.
Prospective observational cohort study.
Six primary and five secondary care sites across South East England, September 2013-November 2015.
One thousand and two hundred and eighty participants, ≥65 years old, who were due for discharge from general medicine and older persons' wards following an acute episode of care. Exclusion criteria were limited life expectancy, transfer to another hospital and consent not gained.
Medication-related harm requiring healthcare utilisation (including primary, secondary or tertiary care consultations related to MRH), including adverse drug reactions, non-adherence and medication error determined via the review of data from three sources: patient/carer reports gathered through a structured telephone interview; primary care medical record review; and prospective consultant-led review of readmission to recruiting hospital. Frailty was measured using a Frailty Index, developed using a standardised approach. Marginal estimates were obtained from logistic regression models to examine how probabilities of healthcare service use due to medication-related harm were associated with increasing number of medicines and frailty.
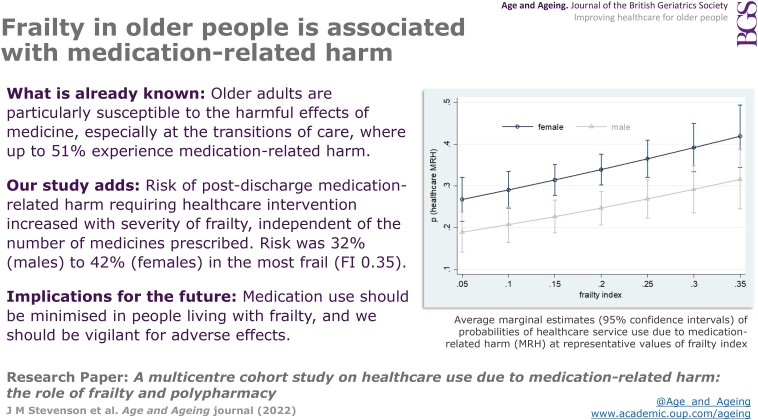
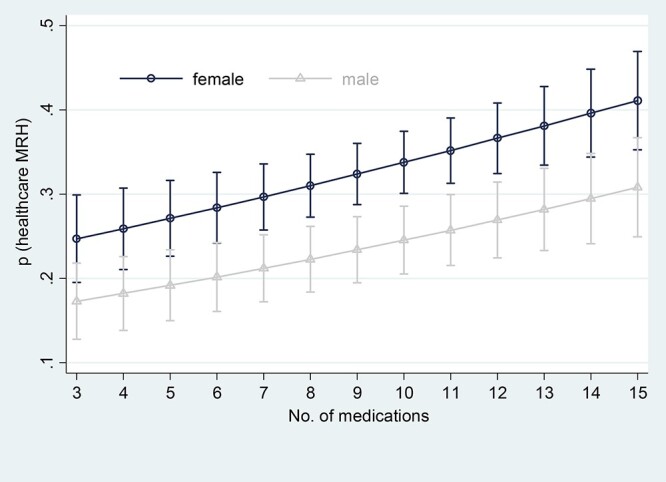
Healthcare utilisation due to medication-related harm was significantly associated with frailty (OR = 10.06, 95% CI 2.06-49.26, P = 0.004), independent of age, gender, and number of medicines. With increasing frailty, the need for healthcare use as a result of MRH increases from a probability of around 0.2-0.4. This is also the case for the number of medicines.
Frailty is associated with MRH, independent of polypharmacy. Reducing the burden of frailty through an integrated health and social care approach, alongside strategies to reduce inappropriate polypharmacy, may reduce MRH related healthcare utilisation.
确定虚弱与需要医疗保健利用的药物相关伤害之间的关联。
前瞻性观察队列研究。
2013 年 9 月至 2015 年 11 月期间,在英格兰东南部的 6 个初级和 5 个二级保健点。
1280 名年龄在 65 岁及以上的参与者,他们在经历了一次急性护理后,将从内科和老年人病房出院。排除标准为预期寿命有限、转院和未获得同意。
需要医疗保健利用的药物相关伤害(包括与 MRH 相关的初级、二级或三级保健咨询),包括药物不良反应、不依从和用药错误,这些是通过审查来自三个来源的数据确定的:通过结构化电话访谈收集的患者/护理人员报告;初级保健医疗记录审查;以及对招募医院重新入院的前瞻性顾问主导审查。虚弱是通过使用标准方法开发的虚弱指数来衡量的。从逻辑回归模型中获得边缘估计,以检查由于药物相关伤害而导致医疗服务使用的概率与使用药物的数量和虚弱程度之间的关系。
药物相关伤害导致的医疗保健利用与虚弱显著相关(OR=10.06,95%CI 2.06-49.26,P=0.004),独立于年龄、性别和药物数量。随着虚弱程度的增加,由于 MRH 而需要医疗保健的可能性从 0.2-0.4 左右增加。这也适用于药物数量。
虚弱与 MRH 相关,与多药治疗无关。通过综合健康和社会保健方法减轻虚弱的负担,同时采取减少不适当多药治疗的策略,可能会减少与 MRH 相关的医疗保健利用。