Department of Emergency Medicine, Wayne State University School of Medicine, Detroit, Michigan, United States of America.
Department of Emergency Medicine, Indiana University School of Medicine, Indianapolis, Indiana, United States of America.
PLoS One. 2022 Mar 31;17(3):e0265895. doi: 10.1371/journal.pone.0265895. eCollection 2022.
Non-invasive finger-cuff monitors measuring cardiac index and vascular tone (SVRI) classify emergency department (ED) patients with acute heart failure (AHF) into three otherwise-indistinguishable subgroups. Our goals were to validate these "hemodynamic profiles" in an external cohort and assess their association with clinical outcomes.
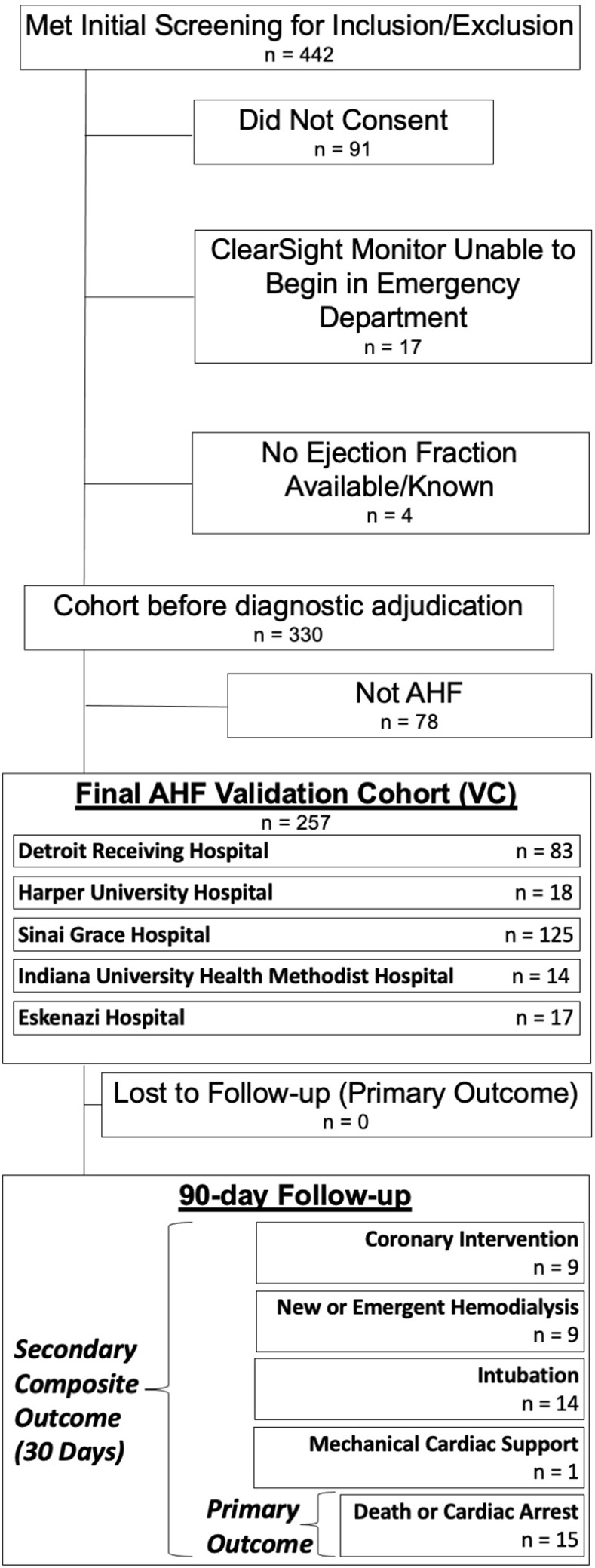
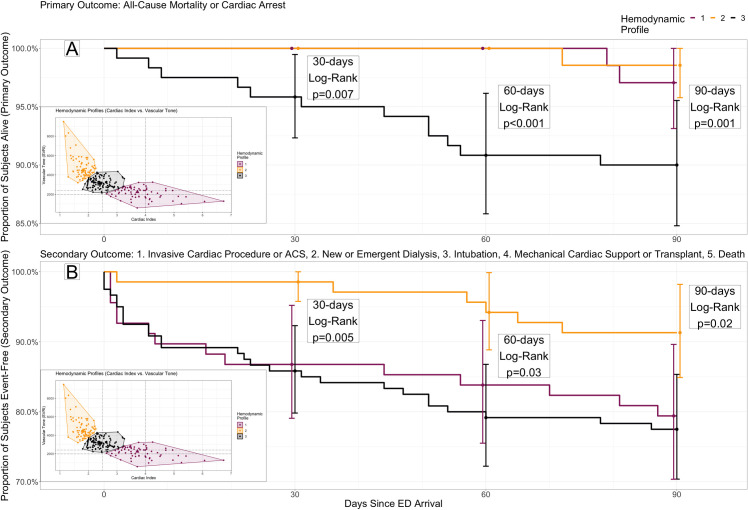
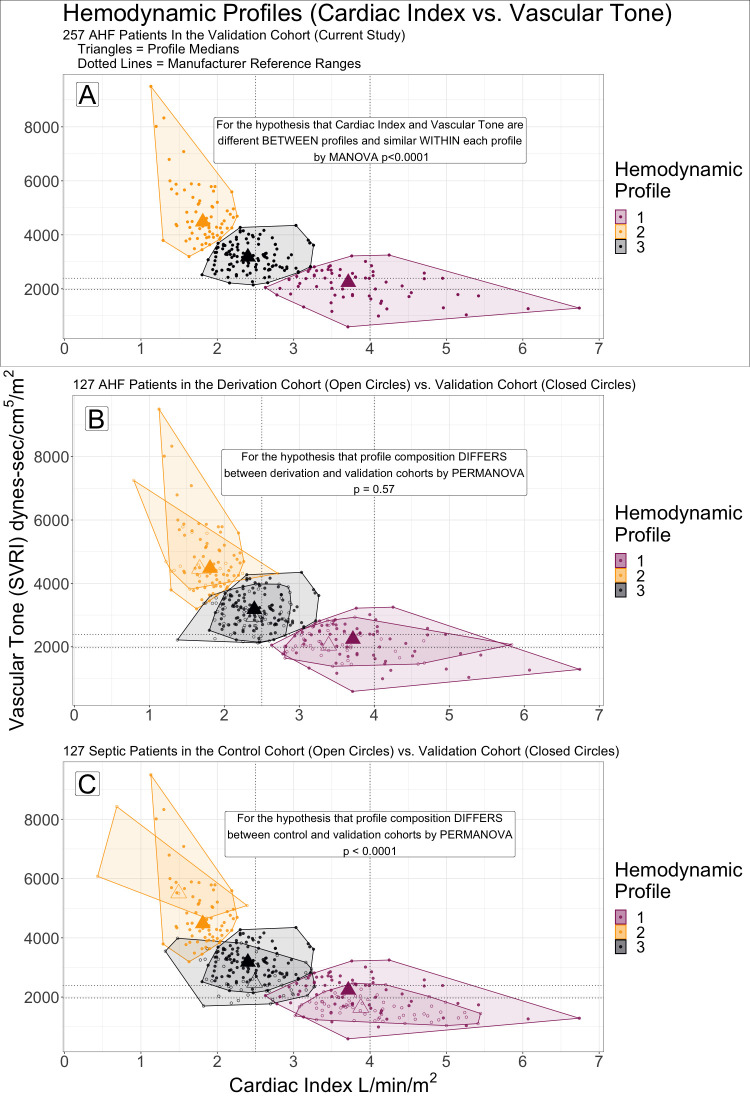
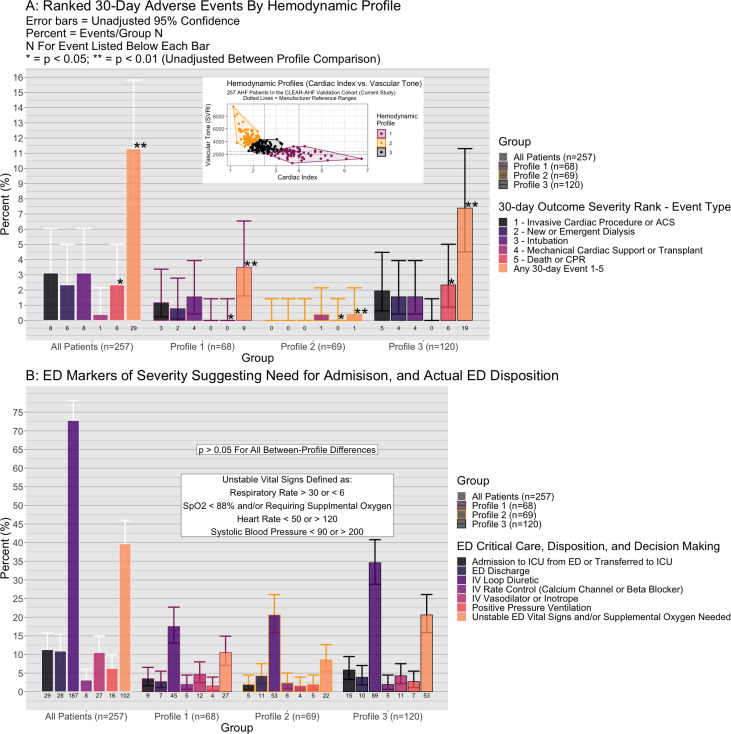
AHF patients (n = 257) from five EDs were prospectively enrolled in the validation cohort (VC). Cardiac index and SVRI were measured with a ClearSight finger-cuff monitor (formerly NexFin, Edwards Lifesciences) as in a previous study (derivation cohort, DC, n = 127). A control cohort (CC, n = 127) of ED patients with sepsis was drawn from the same study as the DC. K-means cluster analysis previously derived two-dimensional (cardiac index and SVRI) hemodynamic profiles in the DC and CC (k = 3 profiles each). The VC was subgrouped de novo into three analogous profiles by unsupervised K-means consensus clustering. PERMANOVA tested whether VC profiles 1-3 differed from profiles 1-3 in the DC and CC, by multivariate group composition of cardiac index and vascular tone. Profiles in the VC were compared by a primary outcome of 90-day mortality and a 30-day ranked composite secondary outcome (death, mechanical cardiac support, intubation, new/emergent dialysis, coronary intervention/surgery) as time-to-event (survival analysis) and binary events (odds ratio, OR). Descriptive statistics were used to compare profiles by two validated risk scores for the primary outcome, and one validated score for the secondary outcome.
The VC had median age 60 years (interquartile range {49-67}), and was 45% (n = 116) female. Multivariate profile composition by cardiac index and vascular tone differed significantly between VC profiles 1-3 and CC profiles 1-3 (p = 0.001, R2 = 0.159). A difference was not detected between profiles in the VC vs. the DC (p = 0.59, R2 = 0.016). VC profile 3 had worse 90-day survival than profiles 1 or 2 (HR = 4.8, 95%CI 1.4-17.1). The ranked secondary outcome was more likely in profile 1 (OR = 10.0, 1.2-81.2) and profile 3 (12.8, 1.7-97.9) compared to profile 2. Diabetes prevalence and blood urea nitrogen were lower in the high-risk profile 3 (p<0.05). No significant differences between profiles were observed for other clinical variables or the 3 clinical risk scores.
Hemodynamic profiles in ED patients with AHF, by non-invasive finger-cuff monitoring of cardiac index and vascular tone, were replicated de novo in an external cohort. Profiles showed significantly different risks of clinically-important adverse patient outcomes.
通过非侵入性指套式监测仪测量心输出量和血管张力(SVRI),可将急诊科(ED)急性心力衰竭(AHF)患者分为三个原本无法区分的亚组。我们的目标是在外部队列中验证这些“血流动力学特征”,并评估它们与临床结局的关系。
从五个 ED 前瞻性纳入 257 例 AHF 患者进入验证队列(VC)。使用 ClearSight 指套式监测仪(前身为 NexFin,爱德华生命科学公司)测量心输出量和 SVRI,与之前的研究(推导队列,DC,n=127)相同。从与 DC 相同的研究中抽取了 ED 败血症患者的对照组(CC,n=127)。先前在 DC 和 CC 中使用 K-均值聚类分析得出了二维(心输出量和 SVRI)血流动力学特征(每个 k=3 个特征)。通过多元组构成的心输出量和血管张力,对 VC 进行了新的无监督 K-均值共识聚类分组。PERMANOVA 测试了 VC 中的 Profile 1-3 是否与 DC 和 CC 中的 Profile 1-3 不同,由心输出量和血管张力的多变量组构成。通过 90 天死亡率和 30 天排名综合次要结局(死亡、机械性心脏支持、插管、新/紧急透析、冠状动脉介入/手术)作为时间事件(生存分析)和二项事件(比值比,OR)比较 VC 中的 Profile。使用两种经过验证的主要结局风险评分和一种经过验证的次要结局评分比较了 Profile。
VC 的中位年龄为 60 岁(四分位距 {49-67}),45%(n=116)为女性。通过心输出量和血管张力的多变量 Profile 组成,VC 的 Profile 1-3 与 CC 的 Profile 1-3 之间存在显著差异(p=0.001,R2=0.159)。但在 VC 与 DC 之间没有检测到 Profile 之间的差异(p=0.59,R2=0.016)。与 Profile 1 或 Profile 2 相比,Profile 3 的 90 天生存率更差(HR=4.8,95%CI 1.4-17.1)。排名较高的次要结局在 Profile 1(OR=10.0,1.2-81.2)和 Profile 3(12.8,1.7-97.9)中比在 Profile 2 中更常见。与高风险 Profile 3 相比,糖尿病患病率和血尿素氮较低(p<0.05)。在其他临床变量或 3 种临床风险评分方面,各 Profile 之间没有观察到显著差异。
通过非侵入性指套式监测仪测量心输出量和血管张力,对 ED 急性心力衰竭患者的血流动力学特征进行了外部队列的重新验证。Profile 显示出明显不同的临床重要不良患者结局风险。