Department of Medicine, Memorial Sloan Kettering Cancer Center, New York City, New York, USA
Department of Medicine, Weill Cornell Medical College, New York City, New York, USA.
J Immunother Cancer. 2022 Apr;10(4). doi: 10.1136/jitc-2021-004149.
Angiosarcoma is a histologically and molecularly heterogeneous vascular neoplasm with aggressive clinical behavior. Emerging data suggests that immune checkpoint blockade (ICB) is efficacious against some angiosarcomas, particularly cutaneous angiosarcoma of the head and neck (CHN).
Patients with histologically confirmed angiosarcoma treated with ICB-based therapy at a comprehensive cancer center were retrospectively identified. Clinical characteristics and the results of targeted exome sequencing, transcriptome sequencing, and immunohistochemistry analyses were examined for correlation with clinical benefit. Durable clinical benefit was defined as a progression-free survival (PFS) of ≥16 weeks.
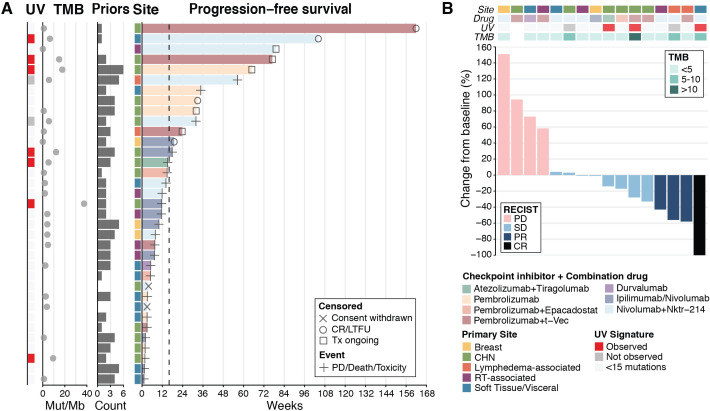
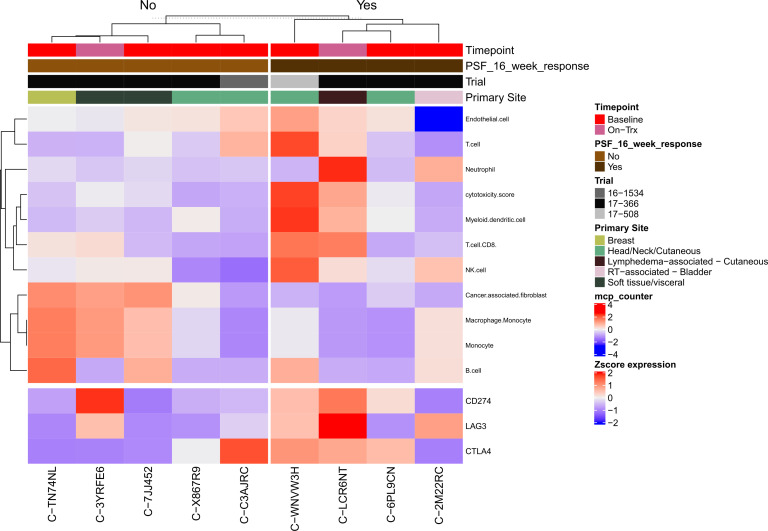
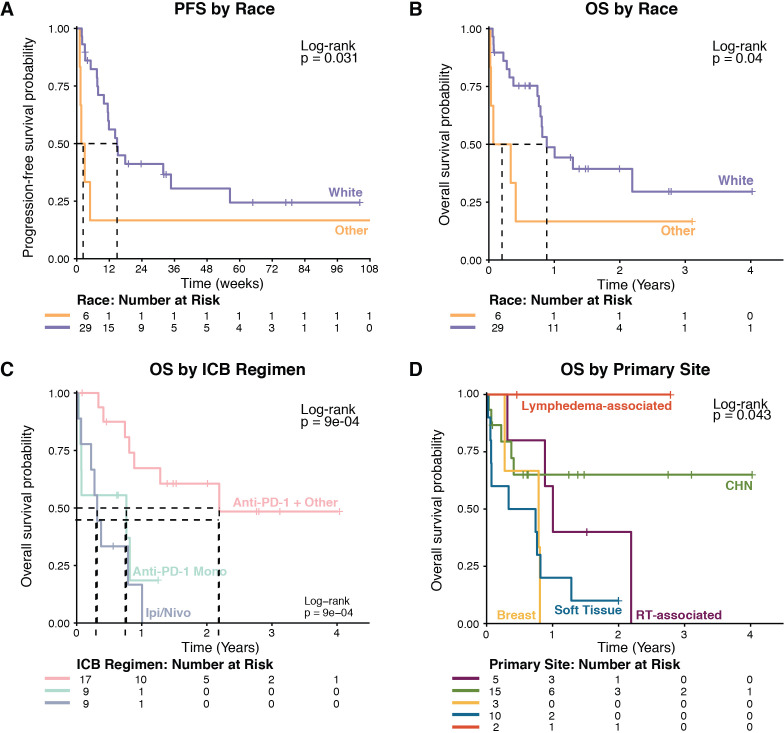
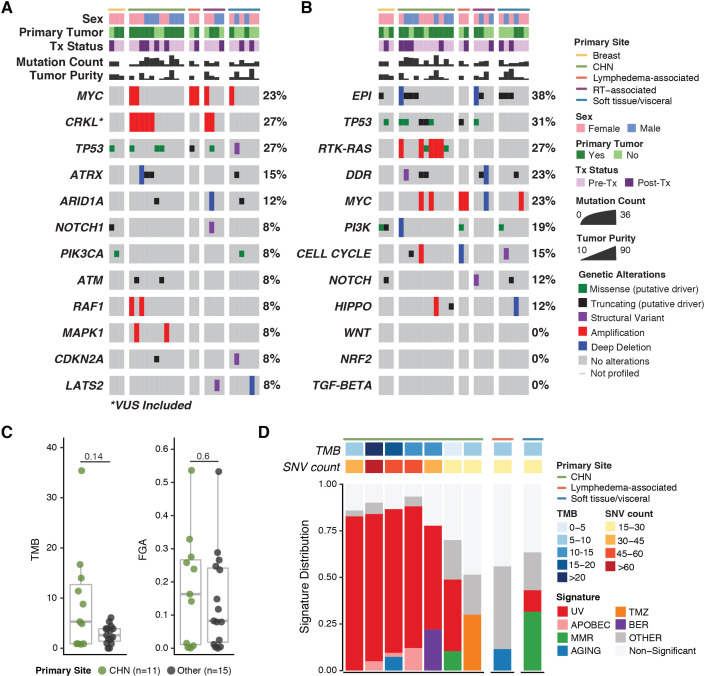
For the 35 patients included in the analyses, median PFS and median overall survival (OS) from the time of first ICB-based treatment were 11.9 (95% CI 7.4 to 31.9) and 42.5 (95% CI 19.6 to 114.2) weeks, respectively. Thirteen patients (37%) had PFS ≥16 weeks. Clinical factors associated with longer PFS and longer OS in multivariate analyses were ICB plus other therapy regimens, CHN disease, and white race. Three of 10 patients with CHN angiosarcoma evaluable for tumor mutational burden (TMB) had a TMB ≥10. Five of six patients with CHN angiosarcoma evaluable for mutational signature analysis had a dominant mutational signature associated with ultraviolet (UV) light. No individual gene or genomic pathway was significantly associated with PFS or OS; neither were TMB or UV signature status. Analyses of whole transcriptomes from nine patient tumor samples found upregulation of angiogenesis, inflammatory response, and KRAS signaling pathways, among others, in patients with PFS ≥16 weeks, as well as higher levels of cytotoxic T cells, dendritic cells, and natural killer cells. Patients with PFS <16 weeks had higher numbers of cancer-associated fibroblasts. Immunohistochemistry findings for 12 patients with baseline samples available suggest that neither PD-L1 expression nor presence of tumor-infiltrating lymphocytes at baseline appears necessary for a response to ICB-based therapy.
ICB-based therapy benefits only a subset of angiosarcoma patients. Patients with CHN angiosarcoma are more likely to have PFS ≥16 weeks, a dominant UV mutational signature, and higher TMB than angiosarcomas arising from other primary sites. However, clinical benefit was seen in other angiosarcomas also and was not restricted to tumors with a high TMB, a dominant UV signature, PD-L1 expression, or presence of tumor infiltrating lymphocytes at baseline.
血管肉瘤是一种组织学和分子上具有异质性的血管肿瘤,具有侵袭性的临床行为。新出现的数据表明,免疫检查点阻断(ICB)对一些血管肉瘤有效,特别是头颈部皮肤血管肉瘤(CHN)。
在一个综合性癌症中心,回顾性地确定了接受基于 ICB 的治疗的组织学证实为血管肉瘤的患者。检查了临床特征以及靶向外显子组测序、转录组测序和免疫组化分析的结果,以与临床获益相关。持久的临床获益定义为无进展生存期(PFS)≥16 周。
在分析中包括的 35 名患者中,从首次 ICB 治疗开始的中位 PFS 和中位总生存期(OS)分别为 11.9(95%CI7.4 至 31.9)和 42.5(95%CI19.6 至 114.2)周。13 名患者(37%)的 PFS≥16 周。多变量分析中与更长 PFS 和 OS 相关的临床因素包括 ICB 加其他治疗方案、CHN 疾病和白种人。10 名 CHN 血管肉瘤患者中有 3 名可评估肿瘤突变负荷(TMB),TMB≥10。6 名 CHN 血管肉瘤患者中有 5 名可评估突变特征分析,有一个与紫外线(UV)相关的主导突变特征。没有一个单独的基因或基因组途径与 PFS 或 OS 显著相关;TMB 或 UV 特征状态也没有。对 9 名患者肿瘤样本的全转录组分析发现,在 PFS≥16 周的患者中,血管生成、炎症反应和 KRAS 信号通路等通路上调,以及细胞毒性 T 细胞、树突状细胞和自然杀伤细胞水平升高。PFS<16 周的患者有更多的癌症相关成纤维细胞。有基线样本的 12 名患者的免疫组化检查结果表明,PD-L1 表达或基线时肿瘤浸润淋巴细胞的存在对于 ICB 治疗的反应都不是必需的。
基于 ICB 的治疗仅使一部分血管肉瘤患者受益。与其他原发部位的血管肉瘤相比,CHN 血管肉瘤患者更有可能出现 PFS≥16 周、主导 UV 突变特征和更高的 TMB。然而,其他血管肉瘤也有临床获益,而且不限于 TMB 高、主导 UV 特征、PD-L1 表达或基线时存在肿瘤浸润淋巴细胞的肿瘤。