Dermatology Department, AP-HP, Henri Mondor Hospital.
Reference Center for Toxic Bullous Diseases and Severe Drug Reactions TOXIBUL, Créteil.
Melanoma Res. 2022 Jun 1;32(3):205-210. doi: 10.1097/CMR.0000000000000819. Epub 2022 Mar 29.
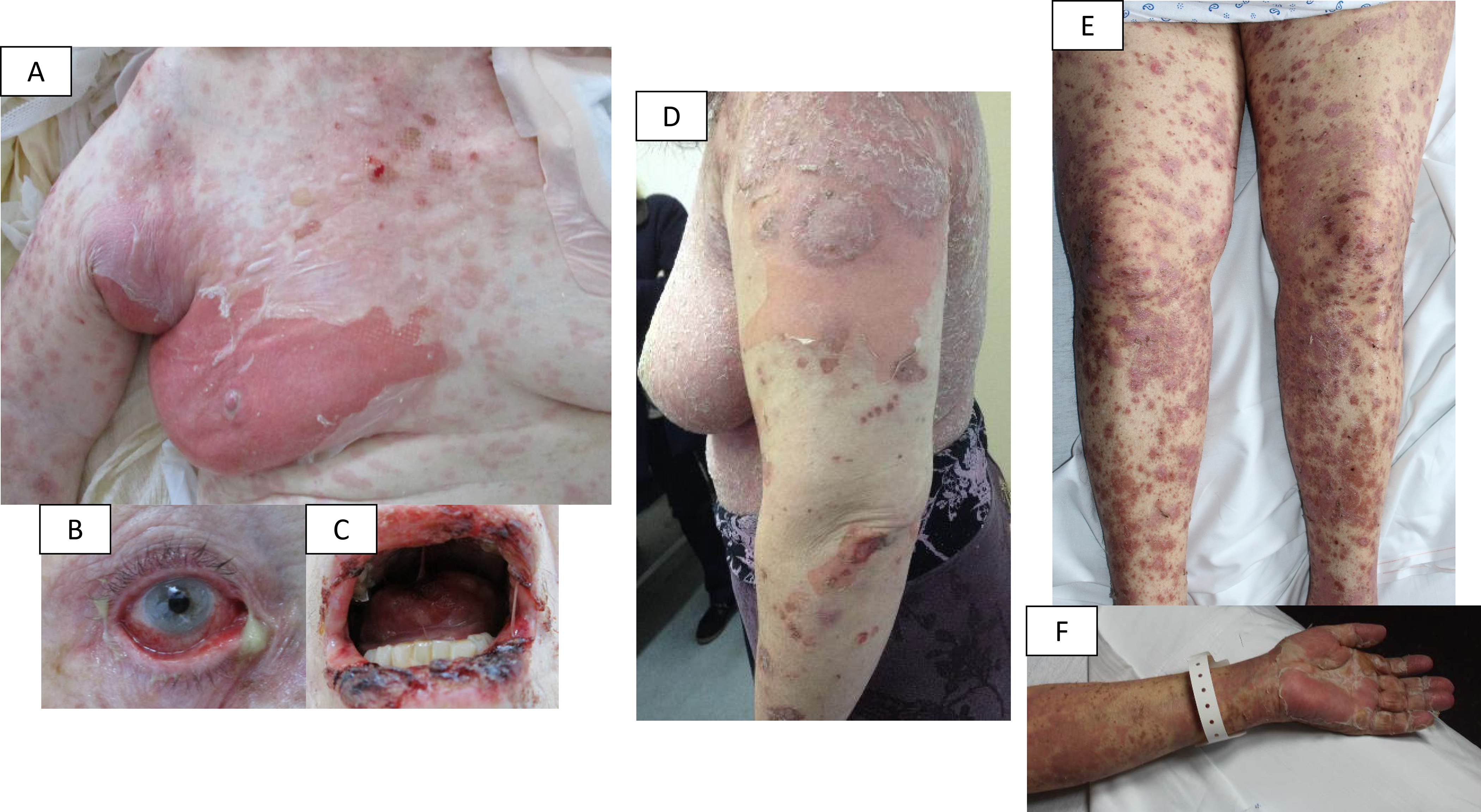
Among dermatologic adverse events induced by immune checkpoint inhibitors (ICI), bullous life-threatening reactions are rare. To better define the clinical and histological features, treatment, and prognosis of ICI-related severe blistering cutaneous eruptions. This retrospective case series was conducted between 2014/05/15 and 2021/04/15 by the dermatology departments of four international registries involved in drug reactions. Inclusion criteria were age ≥18 years old, skin eruption with blisters with detachment covering ≥1% body surface area and at least one mucous membrane involved, available pictures, and ICI as suspect drug. Autoimmune bullous disorders were excluded. Each participant medical team gave his own diagnosis conclusion: epidermal necrolysis (EN), severe lichenoid dermatosis (LD), or unclassified dermatosis (UD). After a standardized review of pictures, cases were reclassified by four experts in EN or LD/UD. Skin biopsies were blindly reviewed. Thirty-two patients were included. Median time to onset was 52 days (3-420 days). Cases were originally diagnosed as EN in 21 cases and LD/UD in 11 cases. After review by experts, 10/21 EN were reclassified as LD/UD. The following manifestations were more frequent or severe in EN: fever, purpuric macules, blisters, ocular involvement, and maximal detachment. Most patients were treated with topical with or without systemic corticosteroids. Eight patients (25%) died in the acute phase. The culprit ICI was not resumed in 92% of cases. In three patients, another ICI was given with a good tolerance. Histology did not reveal significant differences between groups. Severe blistering cutaneous drug reactions induced by ICI are often overdiagnosed as EN. Consensus for management is pending.
在免疫检查点抑制剂 (ICI) 引起的皮肤科不良反应中,危及生命的大疱性反应较为罕见。为了更好地定义 ICI 相关严重水疱性皮肤发疹的临床和组织学特征、治疗和预后,我们开展了此项回顾性病例系列研究,纳入了参与药物不良反应的四个国际登记处的皮肤科部门于 2014 年 5 月 15 日至 2021 年 4 月 15 日期间收治的患者。纳入标准为年龄≥18 岁、皮肤发疹伴有大疱且剥脱面积覆盖≥1%体表面积且至少有一个黏膜受累、有可供使用的图片以及 ICI 为可疑药物。自身免疫性大疱性疾病除外。每位患者的医疗团队都给出了自己的诊断结论:表皮坏死松解症 (EN)、严重的苔藓样皮炎 (LD) 或未分类的皮炎 (UD)。在对图片进行标准化审查后,由 4 名 EN 或 LD/UD 专家对病例进行重新分类。对皮肤活检进行了盲法审查。共纳入 32 例患者。中位发病时间为 52 天(3-420 天)。21 例最初诊断为 EN,11 例最初诊断为 LD/UD。经专家审查后,21 例 EN 中有 10 例被重新分类为 LD/UD。EN 中更常见或更严重的表现包括发热、瘀斑、水疱、眼部受累和最大程度的剥脱。大多数患者接受了局部治疗或局部联合全身皮质类固醇治疗。8 例(25%)在急性期死亡。92%的病例未恢复使用致病的 ICI。在 3 例患者中,另一种 ICI 被给予且具有良好的耐受性。组织学检查未显示两组之间存在显著差异。ICI 引起的严重水疱性皮肤药物反应常被过度诊断为 EN。管理的共识仍有待确定。