Chatain Grégoire P, Kortz Michael W, Serva Stephanie, Shrestha Keshari, Hosokawa Patrick, Ung Timothy H, Finn Michael
Department of Neurosurgery, University of Colorado School of Medicine, Aurora, CO, USA.
Adult and Child Center for Health Outcomes Research and Delivery Science (ACCORDS), University of Colorado, Aurora, CO, USA.
Neurospine. 2022 Mar;19(1):118-132. doi: 10.14245/ns.2143200.600. Epub 2022 Mar 31.
To evaluate how multimodal intraoperative neuromonitoring (IONM) changes during spinal ependymoma (SE) resection correlate with long-term neuro-functional outcomes.
A retrospective analysis of patients aged 18 years or older who underwent surgical resection for SE over a 10-year period was conducted. IONM changes were defined as sustained transcranial motor evoked potential (TcMEP) and/or somatosensory evoked potential (SSEP) signal decrease of 50% or greater from baseline. Primary endpoints were postoperative modified McCormick Neurologic Scale (MNS) scores at postoperative day (POD) < 2, 6 weeks, 1 year, and 2 years. Univariate and multivariate analyses were performed.
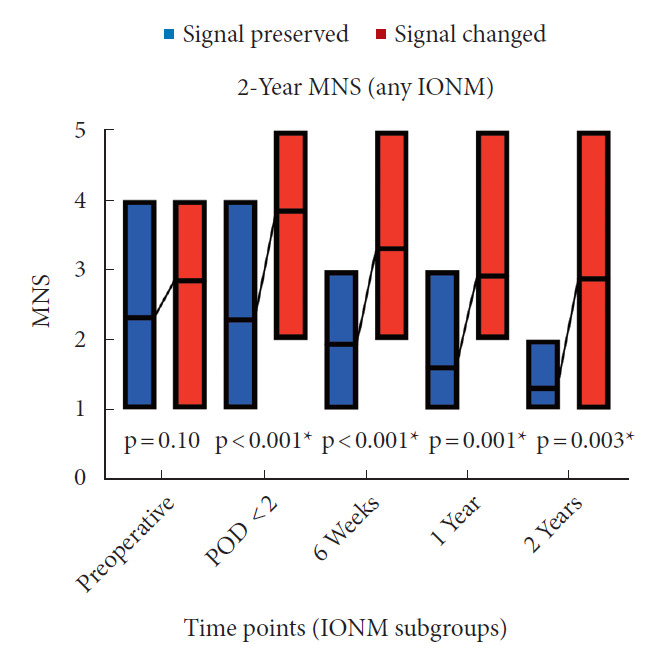
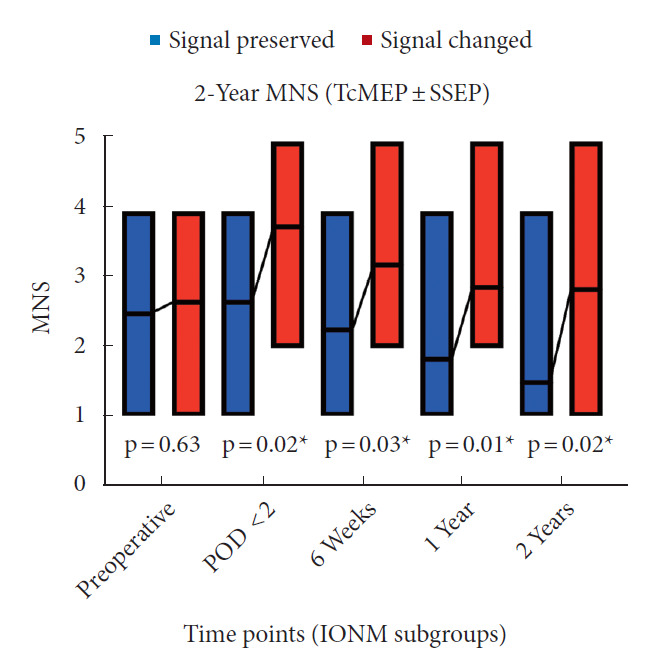
Twenty-nine patients were identified. Average age was 44.2 ± 15.4 years. Sixteen (55.2%) were male and 13 (44.8%) were female. Tumor location was 10 cervical-predominant (34.5%), 13 thoracic-predominant (44.8%), and 6 lumbar/conus-predominant (20.7%). A majority (69.0%) were World Health Organization grade 2 tumors. Twentyfour patients (82.8%) achieved gross total resection. Thirteen patients (44.8%) had a sustained documented IONM signal change and 10 (34.5%) had a TcMEP change with or without derangement in SSEP. At POD < 2, 6 weeks, 1 year, and 2 years, MNS was significantly higher for those when analyzing subgroups with either any sustained IONM or TcMEP ± SSEP signal attenuation > 50% below baseline (all p < 0.05).
Sustained IONM derangements > 50% below baseline, particularly for TcMEP, are significantly associated with higher MNS postoperatively out to 2 years. Intraoperative and postoperative management of these patients warrant special consideration to limit neurologic morbidity.
评估脊柱室管膜瘤(SE)切除术中多模式神经监测(IONM)变化与长期神经功能预后的相关性。
对18岁及以上在10年期间接受SE手术切除的患者进行回顾性分析。IONM变化定义为经颅运动诱发电位(TcMEP)和/或体感诱发电位(SSEP)信号从基线持续下降50%或更多。主要终点是术后第(POD)<2天、6周、1年和2年的术后改良麦考密克神经功能量表(MNS)评分。进行单因素和多因素分析。
共纳入29例患者。平均年龄为44.2±15.4岁。男性16例(55.2%),女性13例(44.8%)。肿瘤部位以颈椎为主10例(34.5%),胸椎为主13例(44.8%),腰椎/圆锥为主6例(20.7%)。大多数(69.0%)为世界卫生组织2级肿瘤。24例患者(82.8%)实现了全切除。13例患者(44.8%)有持续记录的IONM信号变化,10例(34.5%)有TcMEP变化,伴或不伴有SSEP紊乱。在POD<2天、6周、1年和2年时,分析任何持续IONM或TcMEP±SSEP信号衰减>基线以下50%的亚组时,MNS显著更高(所有p<0.05)。
IONM持续紊乱>基线以下50%,尤其是TcMEP,与术后2年更高的MNS显著相关。这些患者的术中和术后管理需要特别考虑以限制神经并发症。