Department of Orthopaedic Surgery, Seoul Now Hospital, Seongnam-si, Gyeonggi, South Korea.
Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam-si, Gyeonggi, South Korea.
BMC Musculoskelet Disord. 2022 Apr 8;23(1):339. doi: 10.1186/s12891-022-05310-z.
This study was performed to evaluate the rebound phenomenon after the correction of coronal angular deformity by hemiepiphysiodesis using tension band plate in children and to identify its risk factors.
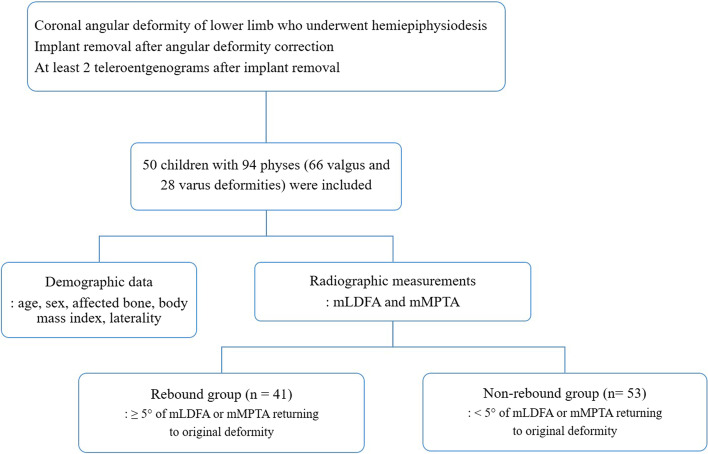
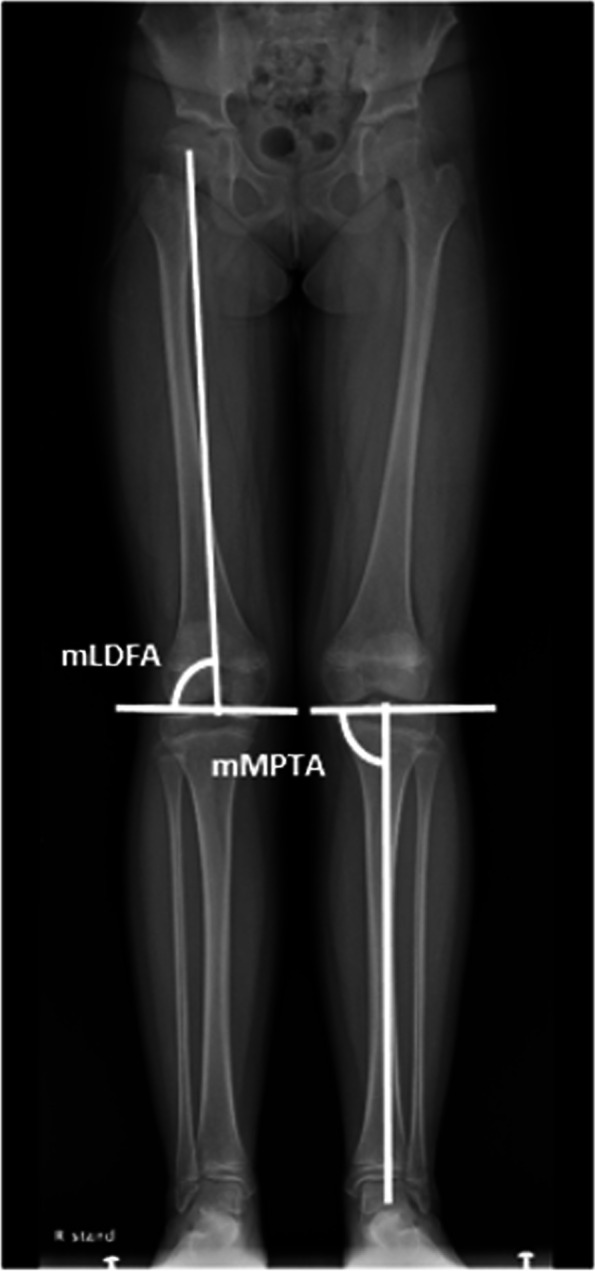
We reviewed 50 children (mean age, 11.0 ± 2.5 years) with 94 physes who had undergone hemiepiphysiodesis using tension band plate due to coronal angular deformity of the lower limb. Patients' demographic data including sex, age at initial surgery and plate removal, affected bone (distal femur or proximal tibia), affected side, and body mass index were collected. The mechanical lateral distal femoral angle (mLDFA) and the mechanical medial proximal tibial angle (mMPTA) were measured from the teleradiogram, Physes were divided into rebound and non-rebound group, and rebound group was defined as the physes which had ≥ 5° of mLDFA or mMPTA returning to its original deformity. Generalized estimating equation based multivariable analysis was used to identify the risk factors for the rebound phenomenon after the deformity correction.
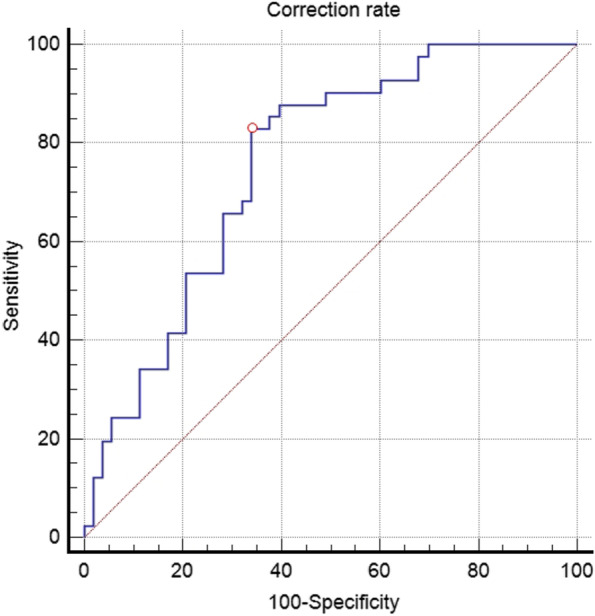
A total of 41 physes classified into rebound group and 53 physes into non-rebound group. There were significant differences in the age at initial surgery (p = 0.004), the age at implant removal (p = 0.002), the amount of correction (p = 0.001), and the rate of correction (p < 0.001) between two groups. The rate of correction was significantly associated with the rebound phenomenon (p = 0.044). The risk of rebound phenomenon was 1.2-fold higher as the rate of correction increased by 1° per year. The cutoff values of the correction rate between the two groups were 6.9°/year (p < 0.001).
This study showed that the rebound group had younger age and faster correction rate than those in the non-rebound group. In addition, the correction rate for deformity was a significant risk factor for the rebound phenomenon after hemiepiphysiodesis using the tension band plate. Close monitoring after implant removal is required for children who have a rapid correction rate over 7°/year.
本研究旨在评估儿童使用张力带钢板行半骺阻滞矫正冠状面角度畸形后出现的反弹现象,并确定其危险因素。
我们回顾了 50 名(平均年龄 11.0±2.5 岁)因下肢冠状面角度畸形接受张力带钢板行半骺阻滞的儿童患者,共 94 个骺板。收集患者的性别、初次手术和钢板取出年龄、受累骨(股骨远端或胫骨近端)、受累侧和体重指数等一般资料。从侧位 X 线片上测量机械性外侧股骨远端角(mLDFA)和机械性内侧胫骨近端角(mMPTA)。骺板分为反弹组和非反弹组,反弹组定义为 mLDFA 或 mMPTA 反弹≥5°,恢复到原有畸形的骺板。采用广义估计方程多变量分析确定畸形矫正后出现反弹现象的危险因素。
共有 41 个骺板归入反弹组,53 个骺板归入非反弹组。两组在初次手术年龄(p=0.004)、钢板取出年龄(p=0.002)、矫正量(p=0.001)和矫正率(p<0.001)方面存在显著差异。矫正率与反弹现象显著相关(p=0.044)。矫正率每年增加 1°,反弹现象的风险增加 1.2 倍。两组间矫正率的临界值为 6.9°/年(p<0.001)。
本研究表明,反弹组的年龄比非反弹组小,矫正速度也更快。此外,畸形的矫正率是张力带钢板行半骺阻滞术后出现反弹现象的显著危险因素。对于矫正率超过 7°/年的儿童,在取出内固定物后需要密切监测。