Department of Laboratory Medicine, Ghent University Hospital, Ghent, Belgium.
Department of General Internal Medicine, Ghent University Hospital, Ghent, Belgium.
Front Immunol. 2022 Mar 22;13:858399. doi: 10.3389/fimmu.2022.858399. eCollection 2022.
Immunocompromised patients are at increased risk of severe COVID-19 and impaired vaccine response. In this observational prospective study, we evaluated immunogenicity of the BNT162b2 mRNA vaccine in cohorts of primary or secondary immunocompromised patients.
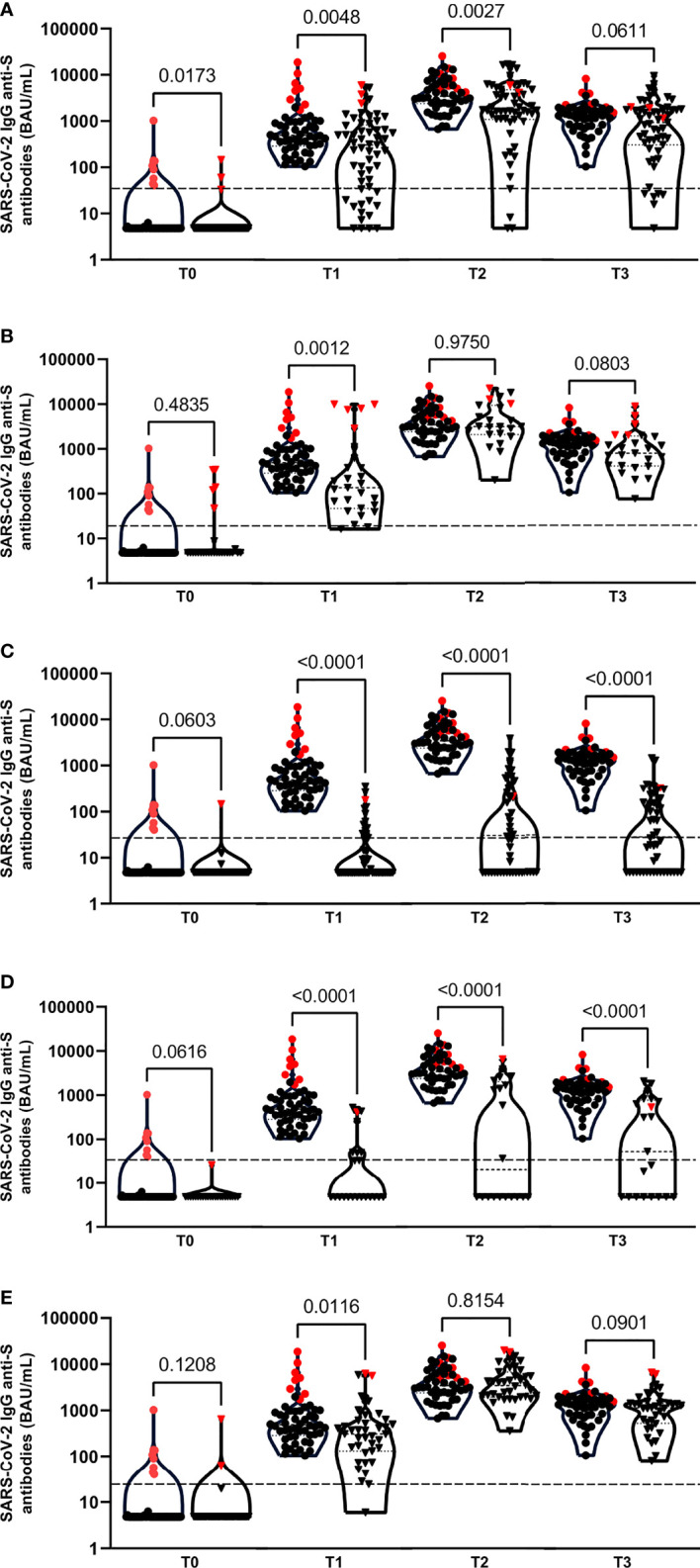
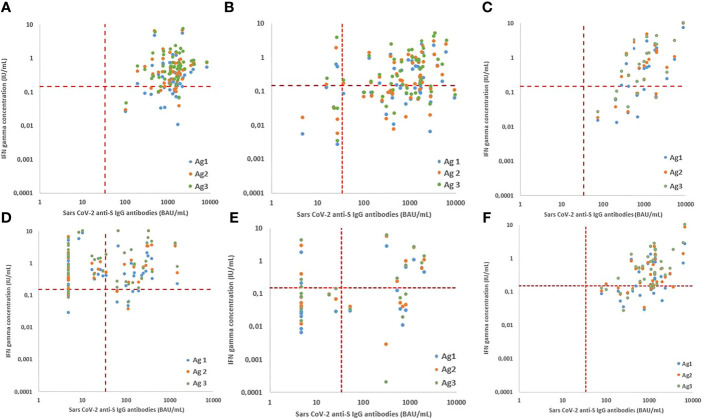
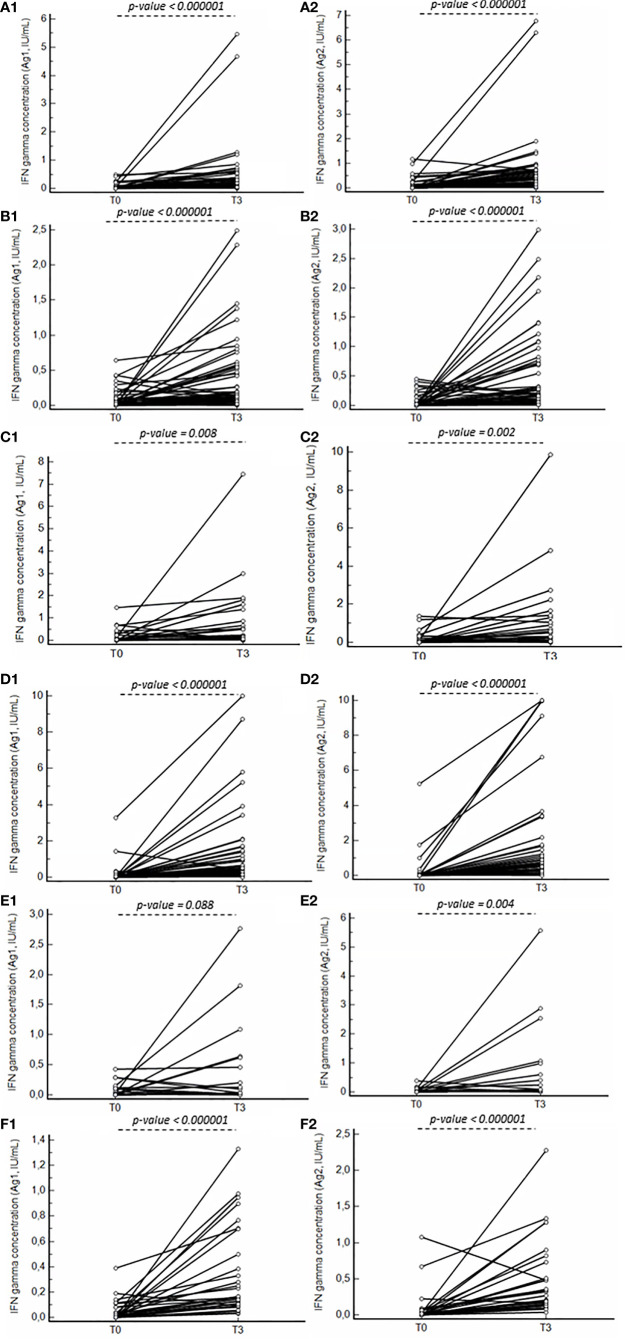
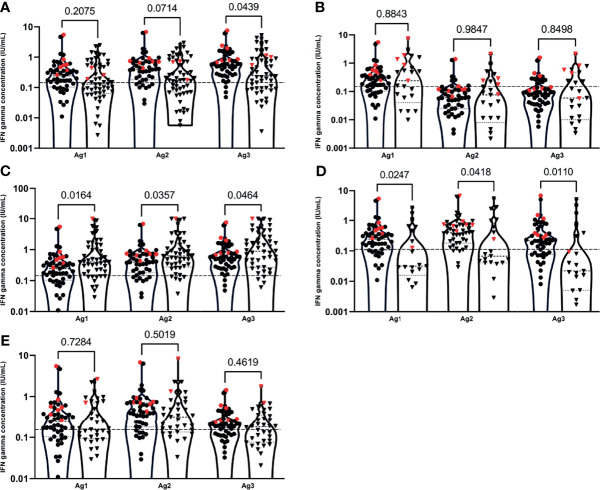
Five clinical groups of immunocompromised patients [primary immunodeficiency (PID) (n=57), people living with HIV (PLWH) (n=27), secondary immunocompromised patients with a broad variety of underlying rheumatologic (n=23) and homogeneous (multiple sclerosis) neurologic (n=53) conditions and chronic kidney disease (CKD) (n=39)] as well as a healthy control group (n=54) were included. Systemic humoral and cellular immune responses were evaluated by determination of anti-SARS-CoV-2 Spike antibodies using a TrimericS IgG assay (Diasorin) and through quantification of interferon gamma release in response to SARS-CoV-2 antigen with QuantiFERON SARS-CoV-2 assay (Qiagen), respectively. Responses were measured at pre-defined time-points after complete vaccination.
All healthy controls, PLWH and CKD-patients had detectable antibodies 10 to 14 days (T2) and 3 months (T3) after administration of the second vaccination. In contrast, only 94.5% of the PID, 50.0% of the rheumatologic and 48.0% of neurologic patients developed antibodies at T2 and only 89.1% of the PID, 52.4% of the rheumatologic and 50.0% of neurologic patients developed antibodies at T3. At T3 no significant differences in cellular response between the healthy control group and the PLWH and CKD groups were found, while proportions of reactive subjects were lower in PID and rheumatologic patients and higher in neurologic patients. Humoral and cellular immune responses significantly correlated in the healthy control, PID, PLWH groups for all 3 antigens.
Patients with acquired or inherited immune disorders may show variable immune responses to vaccination with the BNT162b2 mRNA vaccine against SARS-CoV-2. Whether humoral, cellular or both immune responses are delayed depends on the patient group, therapy and individual risk factors. These data may guide the counselling of patients with immune disorders regarding vaccination of SARS-CoV-2.
免疫功能低下的患者患 COVID-19 重症和疫苗应答受损的风险增加。在这项观察性前瞻性研究中,我们评估了 BNT162b2 mRNA 疫苗在原发性或继发性免疫功能低下患者队列中的免疫原性。
纳入了五个免疫功能低下患者的临床组[原发性免疫缺陷(PID)(n=57)、艾滋病毒感染者(PLWH)(n=27)、广泛的基础风湿性疾病(n=23)和均质(多发性硬化症)神经疾病(n=53)和慢性肾脏病(CKD)(n=39)]以及健康对照组(n=54)。使用 TrimericS IgG 测定法(Diasorin)测定抗 SARS-CoV-2 刺突抗体,通过 QuantiFERON SARS-CoV-2 测定法(Qiagen)定量检测 SARS-CoV-2 抗原刺激后的干扰素γ释放,分别评估全身体液和细胞免疫应答。在完全接种疫苗后的预定时间点测量反应。
所有健康对照者、PLWH 和 CKD 患者在接种第二剂疫苗后 10-14 天(T2)和 3 个月(T3)时均检测到抗体。相比之下,仅 94.5%的 PID、50.0%的风湿性疾病和 48.0%的神经病患者在 T2 时产生了抗体,只有 89.1%的 PID、52.4%的风湿性疾病和 50.0%的神经病患者在 T3 时产生了抗体。在 T3 时,与健康对照组和 PLWH 和 CKD 组相比,细胞反应没有差异,而 PID 和风湿性疾病患者的反应性受试者比例较低,神经病患者的比例较高。在健康对照组、PID 和 PLWH 组中,所有 3 种抗原的体液和细胞免疫反应均显著相关。
获得性或遗传性免疫疾病患者对 BNT162b2 mRNA 疫苗接种 SARS-CoV-2 可能表现出不同的免疫反应。体液、细胞或两者的免疫反应延迟取决于患者群体、治疗和个体危险因素。这些数据可能有助于为免疫功能障碍患者接种 SARS-CoV-2 提供咨询。