Ouyang Yaobin, Zhang Wenjing, He Chen, Zhu Yin, Lu Nonghua, Hu Yi
Department of Gastroenterology, The First Affiliated Hospital of Nanchang University, Nanchang, China.
Medical College of Nanchang University, Nanchang, China.
Front Med (Lausanne). 2022 Mar 24;9:844915. doi: 10.3389/fmed.2022.844915. eCollection 2022.
The increased antibiotic resistance of () has led to the decreased efficacy of regimens.
To evaluate the efficacy, safety, and compliance of susceptibility-guided therapy (SGT) vs. bismuth-containing quadruple therapy (BQT) as the first-line treatment for infection.
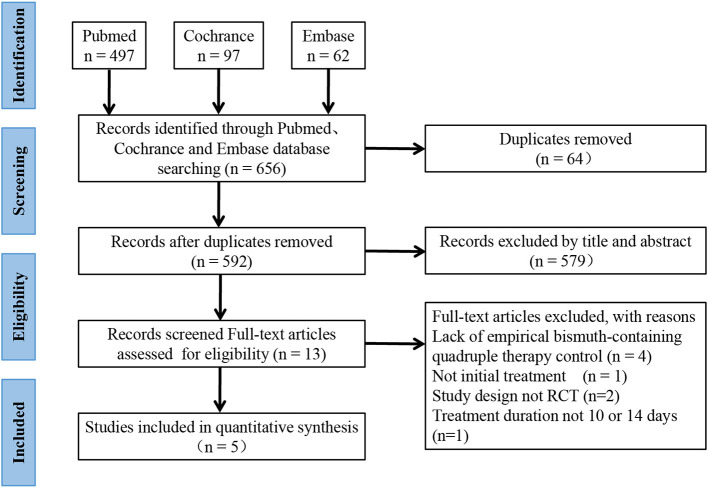
This meta-analysis was performed in accordance with the PRISMA 2009 guidelines. A systematic search in PubMed, Embase, and Cochrane databases was conducted using the combination of " or or ," "bismuth quadruple," and "tailored eradication OR tailored therapy OR susceptibility-guided therapy OR personalized therapy OR antibiotic susceptibility testing."
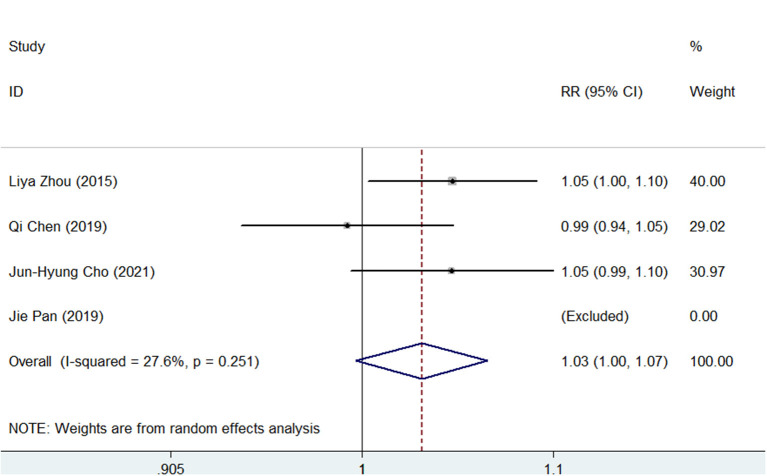
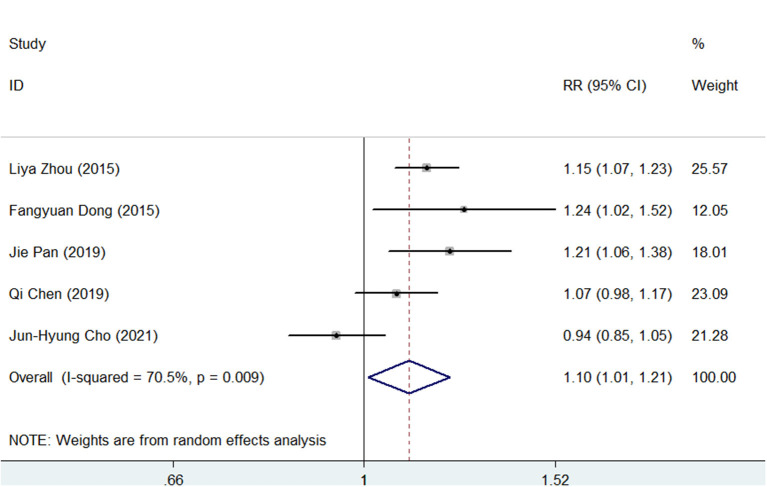
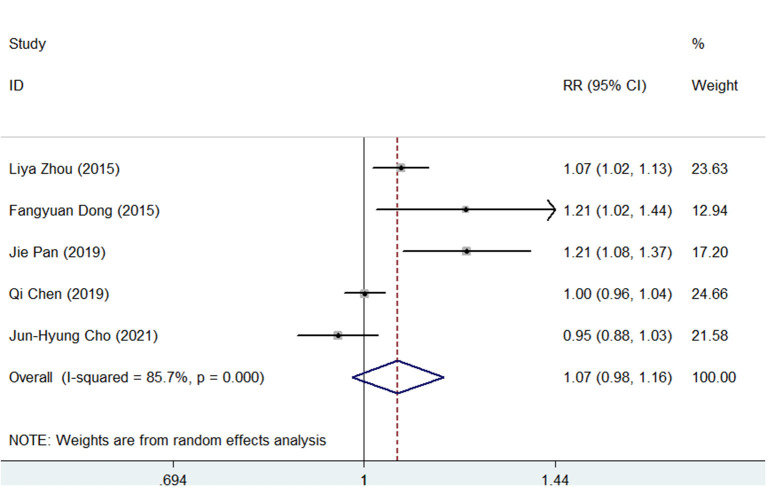
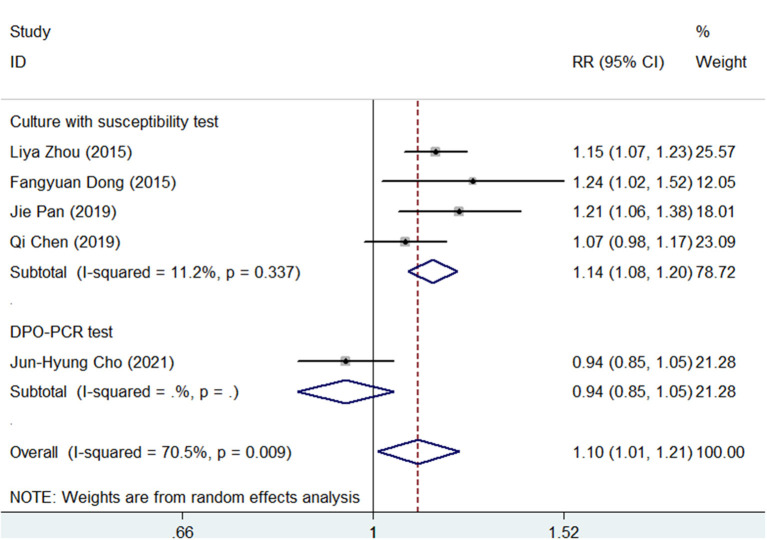
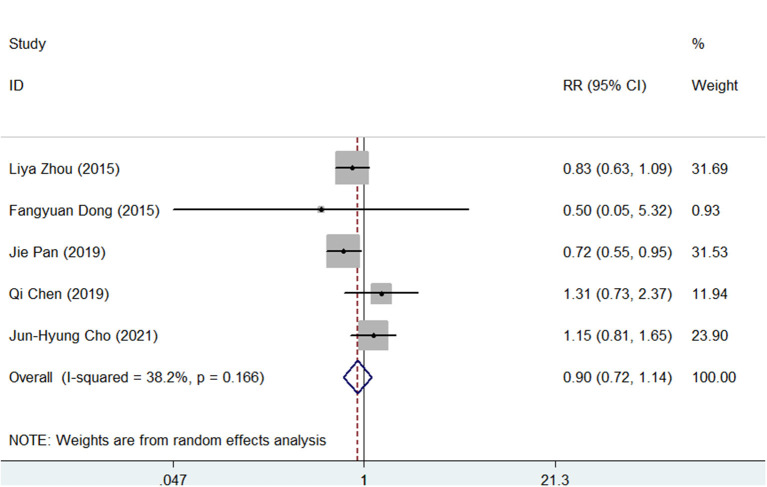
Five studies with 2,110 infected patients were enrolled. The pooled eradication rates of SGT and BQT were 86 vs. 78% ( < 0.05) and 92 vs. 86% ( > 0.05) by intention-to-treat (ITT) and per-protocol (PP) analyses, respectively. SGT has a significantly superior efficacy than BQT [pooled risk ratio (RR) = 1.14, < 0.05] in a subgroup of cultures with the susceptibility test. The pooled side effect rate was 20% in SGT and 22% in BQT, which showed no significant difference ( > 0.05). The compliances of SGT and BQT were 95 and 92%, respectively.
Compared with BQT, SGT showed a higher efficacy and similar safety as the first-line treatment of infection in areas with high antibiotic resistance. The decision-making of first-line regimens for infection should depend on the availability and cost-effectiveness of susceptibility tests and bismuth in local areas.
(某种细菌)抗生素耐药性增加导致(治疗)方案疗效下降。
评估药敏指导治疗(SGT)与含铋四联疗法(BQT)作为(某种细菌)感染一线治疗的疗效、安全性和依从性。
本荟萃分析按照PRISMA 2009指南进行。在PubMed、Embase和Cochrane数据库中进行系统检索,使用“(某种细菌)或(另一种细菌)或(再一种细菌)”、“铋四联”以及“定制根除或定制治疗或药敏指导治疗或个性化治疗或抗生素药敏试验”的组合。
纳入了5项研究,共2110例感染患者。意向性分析(ITT)和符合方案分析(PP)显示,SGT和BQT的根除率分别为86%对78%(P<0.05)和92%对86%(P>0.05)。在进行药敏试验的培养物亚组中,SGT的疗效显著优于BQT[合并风险比(RR)=1.14,P<0.05]。SGT的合并副作用发生率为20%,BQT为22%,差异无统计学意义(P>0.05)。SGT和BQT的依从性分别为95%和92%。
在抗生素耐药性高的地区,与BQT相比,SGT作为(某种细菌)感染的一线治疗显示出更高的疗效和相似的安全性。(某种细菌)感染一线治疗方案的决策应取决于当地药敏试验和铋剂的可获得性及成本效益。