Badreldin Nevert, DiTosto Julia D, Grobman William A, Yee Lynn M
Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Northwestern University School of Medicine, Chicago, Illinois, USA.
Health Equity. 2022 Mar 7;6(1):198-205. doi: 10.1089/heq.2021.0130. eCollection 2022.
To evaluate whether patient-prescriber racial and ethnic concordance is associated with postpartum opioid prescribing patterns and patient-reported pain scores.
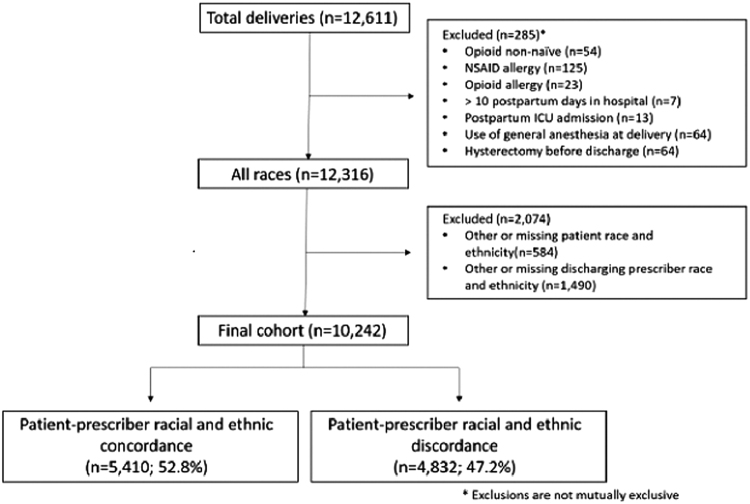
This is a retrospective cohort study of patients who delivered at a tertiary care center between December 1, 2015 and November 30, 2016. Self-identified non-Hispanic white (NHW), non-Hispanic black (NHB), Hispanic, or Asian patients were included. Patient-prescriber pairs were categorized as racially and ethnically concordant if they shared the same racial and ethnic identity; the prescriber was defined as the obstetrical provider who was responsible for the postpartum discharge of the patient. Multivariable regression models controlling for demographic and clinical confounders were used to assess the relationship of patient-prescriber racial and ethnic concordance with receipt of an opioid prescription and patient-reported pain score at discharge.
Of 10,242 patients included in this analysis, 62.3% identified as NHW, 19.1% Hispanic, 9.7% NHB, and 8.9% Asian. About half (52.8%) of patients were discharged by a racially and ethnically concordant prescriber. Patient-prescriber racial and ethnic concordance was not associated with receipt of an opioid prescription (adjusted odds ratio [aOR] 0.82, confidence interval [95% CI] 0.67-1.00) or reporting a pain score ≥5 (aOR 0.90, 95% CI 0.69-1.16). However, NHB and Hispanic patients were less likely to receive an opioid prescription (aOR 0.73, 95% CI 0.56-0.95; aOR 0.73, 95% CI 0.57-0.92, respectively) and significantly more likely to report a pain score ≥5 (aOR 2.13, 95% CI 1.51-3.00; aOR 1.48 95% CI 1.08-2.01, respectively) than NHW patients, even when accounting for concordance.
Disparities in postpartum opioid prescribing and pain perception are not ameliorated by patient-prescriber racial and ethnic concordance.
评估患者与开处方者的种族和民族一致性是否与产后阿片类药物处方模式及患者报告的疼痛评分相关。
这是一项对2015年12月1日至2016年11月30日在一家三级医疗中心分娩的患者进行的回顾性队列研究。纳入自我认定的非西班牙裔白人(NHW)、非西班牙裔黑人(NHB)、西班牙裔或亚裔患者。如果患者与开处方者具有相同的种族和民族身份,则将其配对归类为种族和民族一致;开处方者定义为负责患者产后出院的产科医护人员。使用控制人口统计学和临床混杂因素的多变量回归模型来评估患者与开处方者的种族和民族一致性与阿片类药物处方的开具以及出院时患者报告的疼痛评分之间的关系。
在纳入本次分析的10242名患者中,62.3%为非西班牙裔白人,19.1%为西班牙裔,9.7%为非西班牙裔黑人,8.9%为亚裔。约一半(52.8%)的患者由种族和民族一致的开处方者办理出院手续。患者与开处方者的种族和民族一致性与阿片类药物处方的开具(校正比值比[aOR]0.82,置信区间[95%CI]0.67 - 1.00)或报告疼痛评分≥5(aOR 0.90,95%CI 0.69 - 1.16)无关。然而,即使考虑到一致性,非西班牙裔黑人和西班牙裔患者接受阿片类药物处方的可能性较小(aOR分别为0.73,95%CI 0.56 - 0.95;aOR 0.73,95%CI 0.57 - 0.92),且报告疼痛评分≥5的可能性显著高于非西班牙裔白人患者(aOR分别为2.13,95%CI 1.51 - 3.00;aOR 1.48,95%CI 1.08 - 2.01)。
患者与开处方者的种族和民族一致性并不能改善产后阿片类药物处方和疼痛感知方面的差异。