Istl Alexandra C, Gronchi Alessandro
Division of Surgical Oncology, Johns Hopkins Hospital, Baltimore, MD 21287, USA.
Department of Surgery, Fondazione IRCCS Istituto Nazionale dei Tumori, Via Venezian 1, 20133 Milan, Italy.
Cancers (Basel). 2022 Apr 5;14(7):1831. doi: 10.3390/cancers14071831.
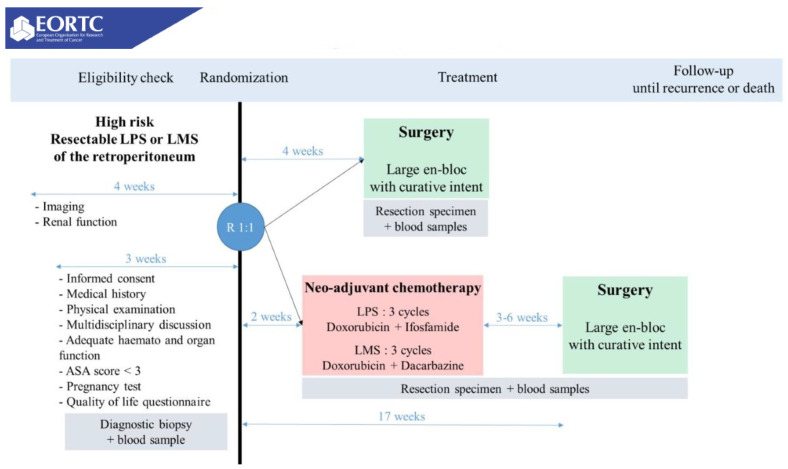
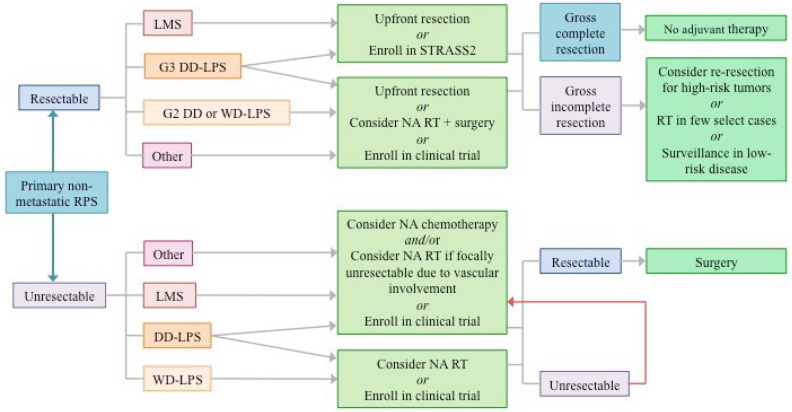
The cornerstone of therapy for primary retroperitoneal sarcomas (RPS) is complete surgical resection, best achieved by resecting the tumor en bloc with adherent structures even if not overtly infiltrated. Until recently, trials designed to elucidate the role of neoadjuvant radiation or chemotherapy for RPS have been unable to achieve sufficient enrollment. The completion of the STRASS trial, which explored neoadjuvant radiotherapy for primary resectable RPS, is a major milestone in RPS research, but has prompted further questions about histology-driven treatment paradigms for RPS. Though it was ultimately a negative trial with respect to its primary endpoint of abdominal recurrence-free survival, STRASS produced a signal that suggested improved abdominal recurrence-free survival with neoadjuvant radiotherapy (RT) for patients with liposarcoma (LPS). No effect was seen for leiomyosarcoma (LMS) or high-grade dedifferentiated (DD) LPS, consistent with recent literature suggesting LMS and high-grade DD-LPS have a predominant pattern of distant rather than local failure. These results, along with those from other recent studies conducted at the bench and the bedside, emphasize the importance of a histology-specific approach to RPS research. Recent evidence for patterns of distant failure in LMS and high-grade DD-LPS has prompted the initiation of STRASS2, a study of neoadjuvant chemotherapy for these histologies. As this study unfolds, evidence may emerge for novel systemic therapy options in specific sarcoma histotypes given the explosion in targeted and immunotherapeutic applications over the last decade. This article reviews current and recent evidence around neoadjuvant radiation and chemotherapy as well as avenues for future study to optimize these treatment approaches.
原发性腹膜后肉瘤(RPS)治疗的基石是完整的手术切除,最好的方法是将肿瘤与粘连结构整块切除,即使没有明显浸润。直到最近,旨在阐明新辅助放疗或化疗对RPS作用的试验仍未能招募到足够的患者。探索原发性可切除RPS新辅助放疗的STRASS试验的完成是RPS研究的一个重要里程碑,但也引发了关于RPS组织学驱动治疗模式的进一步问题。尽管STRASS在其主要终点腹部无复发生存方面最终是一项阴性试验,但它产生了一个信号,表明新辅助放疗(RT)可改善脂肪肉瘤(LPS)患者的腹部无复发生存。平滑肌肉瘤(LMS)或高级别去分化(DD)LPS未观察到效果,这与最近的文献一致,表明LMS和高级别DD-LPS主要表现为远处而非局部失败。这些结果,以及最近在实验室和床边进行的其他研究结果,强调了RPS研究中组织学特异性方法的重要性。最近关于LMS和高级别DD-LPS远处失败模式的证据促使启动了STRASS2,这是一项针对这些组织学的新辅助化疗研究。随着这项研究的展开,鉴于过去十年靶向和免疫治疗应用的激增,可能会出现针对特定肉瘤组织学类型的新型全身治疗选择的证据。本文综述了关于新辅助放疗和化疗的当前及最新证据,以及未来优化这些治疗方法的研究途径。