Department of Surgical Gastroenterology, Centre for Cancer and Organ Diseases, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
Department of Anaesthesia, Centre for Cancer and Organ Diseases, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
J Clin Monit Comput. 2023 Feb;37(1):63-70. doi: 10.1007/s10877-022-00857-7. Epub 2022 Apr 16.
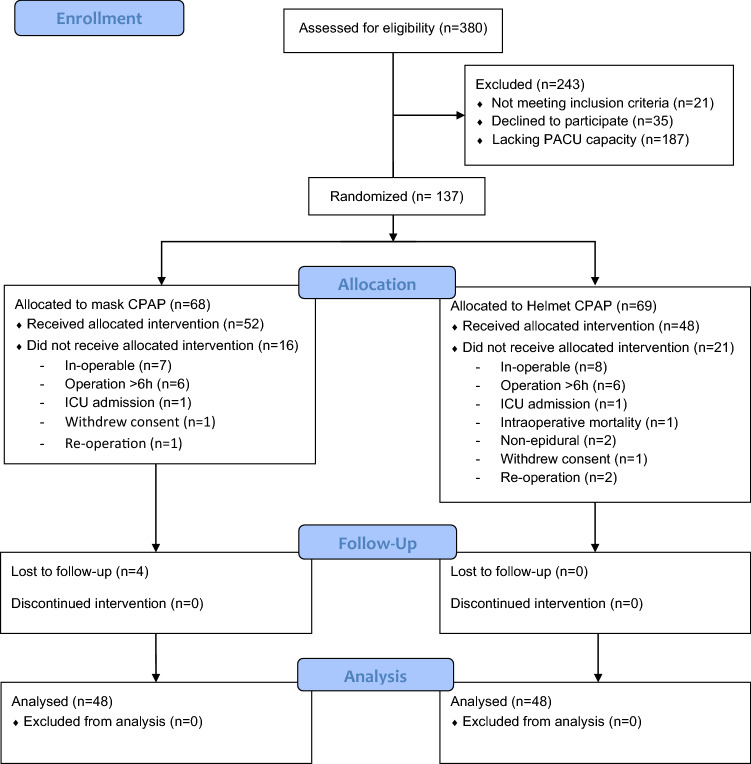
The risk of pulmonary complications is high after major abdominal surgery but may be reduced by prophylactic postoperative noninvasive ventilation using continuous positive airway pressure (CPAP). This study compared the effects of intermittent mask CPAP (ICPAP) and continuous helmet CPAP (HCPAP) on oxygenation and the risk of pulmonary complications following major abdominal surgery. Patients undergoing open abdominal aortic aneurysm repair or pancreaticoduodenectomy were randomized (1:1) to either postoperative ICPAP or HCPAP. Oxygenation was evaluated as the partial pressure of oxygen in arterial blood fraction of inspired oxygen ratio (PaO/FIO) at 6 h, 12 h, and 18 h postoperatively. Pulmonary complications were defined as X-ray verified pneumonia/atelectasis, clinical signs of pneumonia, or supplementary oxygen beyond postoperative day 3. Patient-reported comfort during CPAP treatment was also evaluated. In total, 96 patients (ICPAP, n = 48; HCPAP, n = 48) were included, and the type of surgical procedure were evenly distributed between the groups. Oxygenation did not differ between the groups by 6 h, 12 h, or 18 h postoperatively (p = 0.1, 0.08, and 0.67, respectively). Nor was there any difference in X-ray verified pneumonia/atelectasis (p = 0.40) or supplementary oxygen beyond postoperative day 3 (p = 0.53). Clinical signs of pneumonia tended to be more frequent in the ICPAP group (p = 0.06), yet the difference was not statistically significant. Comfort scores were similar in both groups (p = 0.43), although a sensation of claustrophobia during treatment was only experienced in the HCPAP group (11% vs. 0%, p = 0.03). Compared with ICPAP, using HCPAP was associated with similar oxygenation (i.e., PaO/FIO ratio) and a similar risk of pulmonary complications. However, HCPAP treatment was associated with a higher sensation of claustrophobia.
全麻腹部手术后肺部并发症风险较高,但采用持续气道正压通气(CPAP)进行预防性术后无创通气可降低风险。本研究比较了间歇面罩 CPAP(ICPAP)和连续头盔 CPAP(HCPAP)对全麻腹部手术后氧合和肺部并发症风险的影响。行开放性腹主动脉瘤修复术或胰十二指肠切除术的患者按 1:1 随机分配至术后 ICPAP 或 HCPAP 组。术后 6、12 和 18 小时评估氧合情况,即动脉血氧分压与吸入氧分数比(PaO/FIO)。肺部并发症定义为 X 射线证实的肺炎/肺不张、肺炎临床体征或术后第 3 天以上需要补充吸氧。还评估了 CPAP 治疗期间患者的舒适度。共纳入 96 例患者(ICPAP 组 n=48;HCPAP 组 n=48),两组手术类型分布均匀。术后 6、12 和 18 小时时两组患者的氧合情况无差异(p=0.1、0.08 和 0.67)。X 射线证实的肺炎/肺不张(p=0.40)或术后第 3 天以上需要补充吸氧(p=0.53)也无差异。ICPAP 组肺炎临床体征更常见(p=0.06),但差异无统计学意义。两组舒适度评分相似(p=0.43),但 HCPAP 组治疗时仅 11%的患者有幽闭恐惧症感觉(0%,p=0.03)。与 ICPAP 相比,HCPAP 治疗与相似的氧合(即 PaO/FIO 比值)和相似的肺部并发症风险相关。但 HCPAP 治疗时幽闭恐惧症感觉更常见。