Sattler Samantha S, Magro Cynthia M, Shapiro Lee, Merves Jamie F, Levy Rebecca, Veenstra Jesse, Patel Puraj
Albany Medical College, Albany, NY, USA.
Department of Pathology and Laboratory Medicine, Weill Cornell Medicine, New York, NY, USA.
Orphanet J Rare Dis. 2022 Apr 20;17(1):172. doi: 10.1186/s13023-022-02322-9.
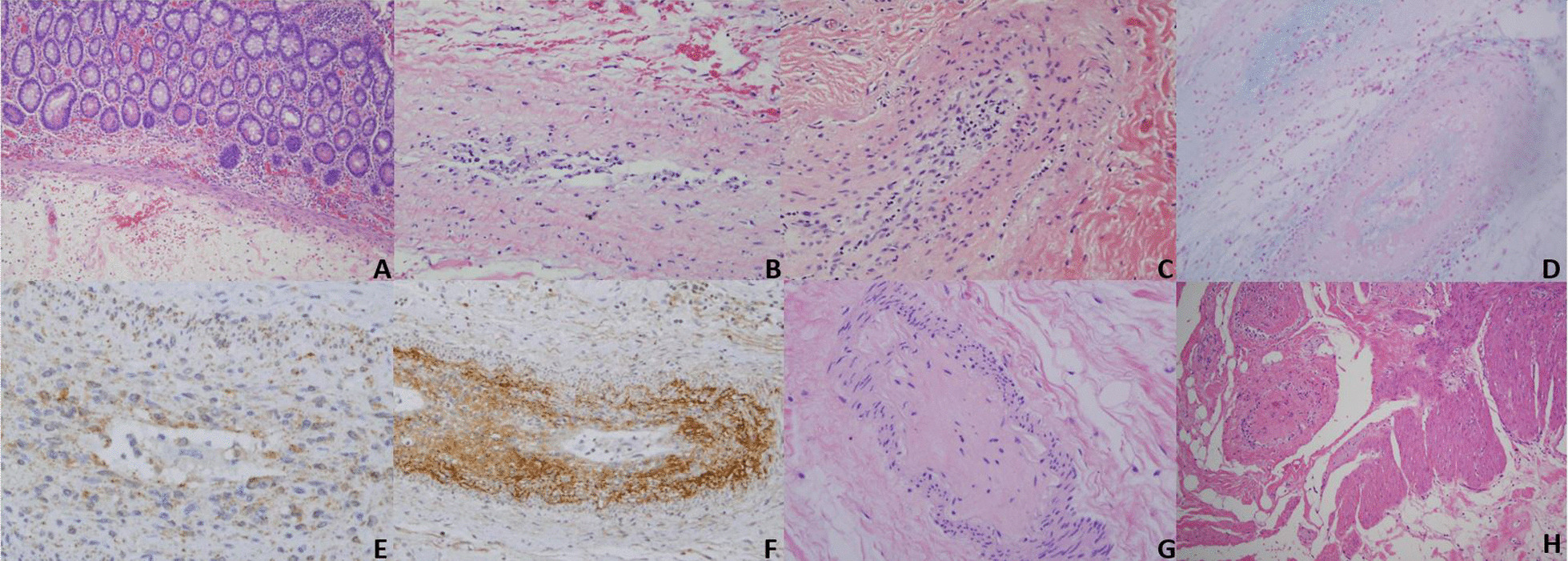
Kohlmeier-Degos (K-D) disease is a rare obliterative vasculopathy that can present as a benign cutaneous form or with potentially malignant systemic involvement. The gastrointestinal tract is most frequently involved in systemic disease and mortality is often related to bowel perforations. Herein, we provide information to providers and patients regarding gastrointestinal K-D symptomology, pathology, treatment, and diagnosis, with a focus on the importance of timely diagnostic laparoscopy. We present three new cases of gastrointestinal K-D to highlight varying disease presentations and outcomes. BODY: Based on reviewed reports, perforation is preceded by at least one gastrointestinal symptom: abdominal pain/cramping, anorexia/weight loss, vomiting, diarrhea, nausea, gastrointestinal bleeding, obstipation, constipation, and abdominal fullness. Perforation most commonly occurs in the small intestine and often results in sepsis and death. Although underutilized, laparoscopy is the most sensitive and specific diagnostic technique, demonstrating serosal porcelain plaques similar to those on the skin and characteristic for K-D. The combination of eculizumab and treprostinil is presently the most effective treatment option for gastrointestinal K-D. The pathology of gastrointestinal K-D is characterized by an obliterative intimal arteriopathy eventuating in occlusive acellular deposits of mucin and collagen along with an extravascular pauci-cellular sclerosing process resembling scleroderma confined to the subserosal fat. C5b-9 and interferon-alpha are both expressed in all caliber of vessels in the affected intestine. While C5b-9 blockade does not prevent the intimal expansion, enhanced type I interferon signaling is likely a key determinant to intimal expansion by, causing an influx of monocytes which transdifferentiate into procollagen-producing myofibroblast-like cells.
Prompt laparoscopic evaluation is necessary in any K-D patient with an abdominal symptom to facilitate diagnosis and treatment initiation, as well as to hopefully decrease mortality. Those with gastrointestinal K-D should start on eculizumab as soon as possible, as onset of action is immediate.
科尔迈尔 - 德戈斯(K-D)病是一种罕见的闭塞性血管病,可表现为良性皮肤形式或伴有潜在恶性的全身受累。胃肠道是全身疾病最常累及的部位,死亡率通常与肠穿孔有关。在此,我们向医疗服务提供者和患者提供有关胃肠道K-D的症状、病理、治疗和诊断的信息,重点强调及时进行诊断性腹腔镜检查的重要性。我们报告三例新的胃肠道K-D病例,以突出不同的疾病表现和结局。
根据已审查的报告,穿孔之前至少会出现一种胃肠道症状:腹痛/绞痛、厌食/体重减轻、呕吐、腹泻、恶心、胃肠道出血、排便困难、便秘和腹部胀满。穿孔最常发生在小肠,常导致败血症和死亡。尽管腹腔镜检查未得到充分利用,但它是最敏感和特异的诊断技术,可显示与皮肤上相似的浆膜瓷样斑块,这是K-D的特征。依库珠单抗和曲前列尼尔联合使用目前是治疗胃肠道K-D最有效的选择。胃肠道K-D的病理特征是闭塞性内膜动脉病,最终导致粘蛋白和胶原蛋白的无细胞闭塞性沉积,以及类似于局限于浆膜下脂肪的硬皮病的血管外少细胞硬化过程。C5b-9和干扰素-α在受影响肠道的所有管径血管中均有表达。虽然C5b-9阻断不能阻止内膜扩张,但增强的I型干扰素信号可能是内膜扩张的关键决定因素,它会导致单核细胞流入,这些单核细胞转分化为产生前胶原的肌成纤维细胞样细胞。
对于任何有腹部症状的K-D患者,及时进行腹腔镜评估对于促进诊断和开始治疗以及有望降低死亡率是必要的。患有胃肠道K-D的患者应尽快开始使用依库珠单抗,因为其起效迅速。