Na Kun, Qiu Miaohan, Ma Sicong, Li Yi, Li Jing, Liu Rong, Zhang Jiaoyang, Han Yaling
School of Life Science and Biochemistry, Shenyang Pharmaceutical University, Shenyang, China.
Department of Cardiology, General Hospital of Northern Theater Command, Shenyang, China.
Front Cardiovasc Med. 2022 Apr 4;9:808571. doi: 10.3389/fcvm.2022.808571. eCollection 2022.
The clinical benefit of ticagrelor vs. clopidogrel in unselected patients with acute coronary syndrome (ACS) after percutaneous coronary intervention (PCI) remains controversial in the real world. This study was aimed to investigate the impact of ticagrelor vs. clopidogrel in subjects with ACS without atrial fibrillation or flutter (AF) after PCI based on risk stratification using the CHADS-VASc score.
In 2016-2019, patients who underwent PCI with at least one stent implanted in the General Hospital of Northern Theater Command were classified as low- or high-risk groups according to the CHADS-VASc score. Incidences of 12-month ischemia [cardiac death, myocardial infarction (MI), or stroke], all-cause death, Bleeding Academic Research Consortium (BARC) 2,3,5 bleeding, BARC 3,5 bleeding, and net adverse clinical events (NACEs) (all-cause death, MI, stroke, or BARC 3, 5 bleeding) with aspirin plus different P2Y inhibitors (clopidogrel or ticagrelor) were appraised among different risk groups. Propensity score matching (PSM) and Cox multivariate analysis were used to balance the groups.
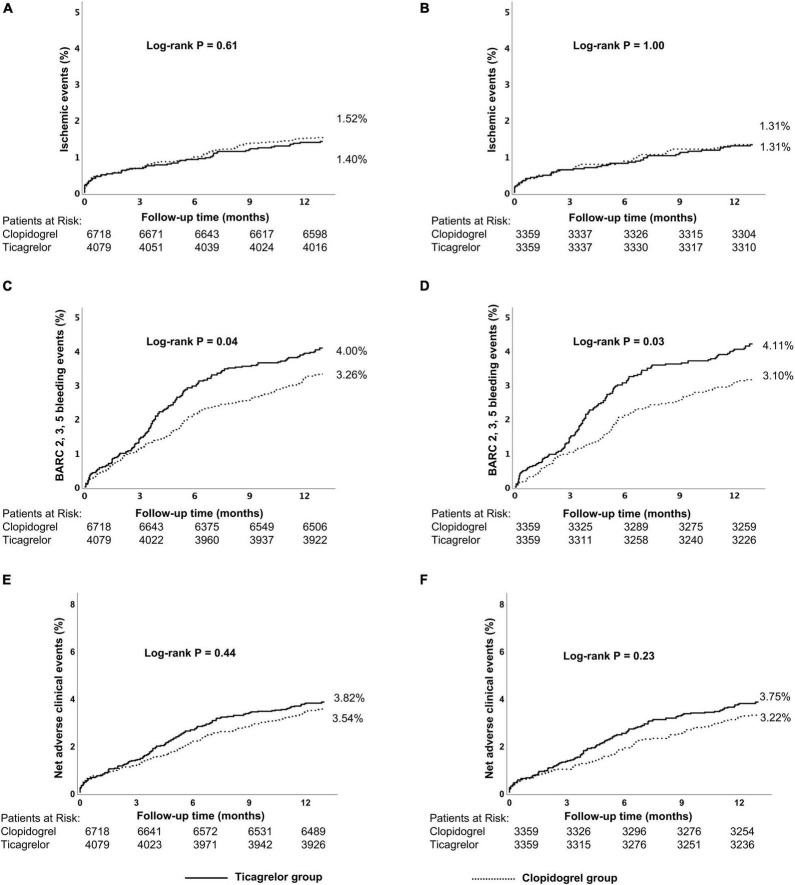
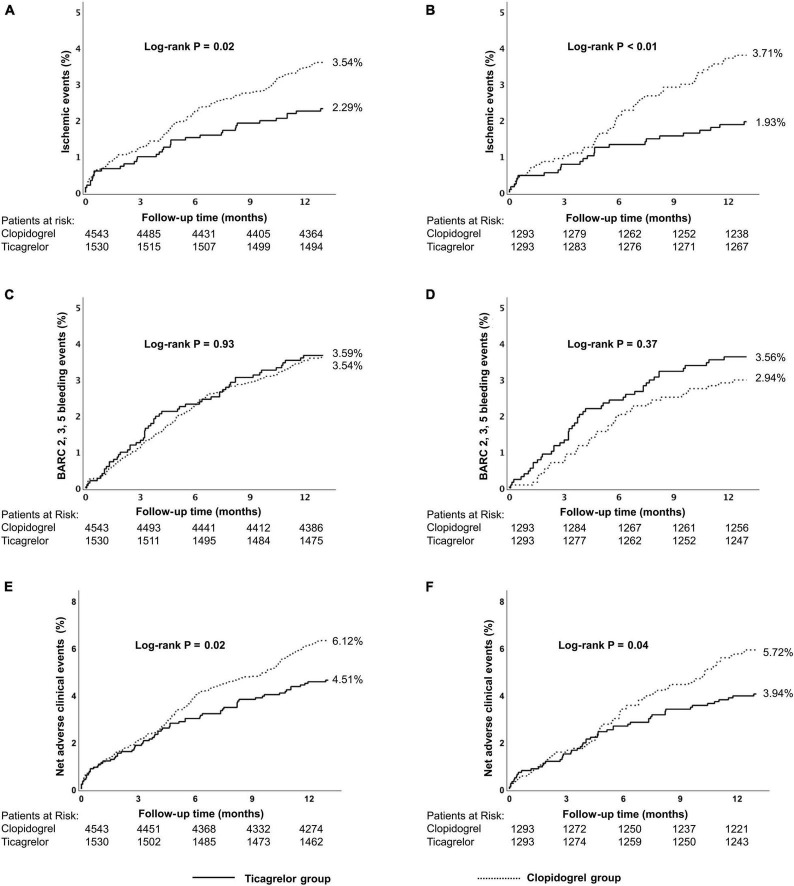
A total of consecutive 17,037 patients with ACS were enrolled. The optimal cut-off value of the CHADS-VASc score for ischemic events by the Youden test was 3 points. Among patients with high risk (CHADS-VASc ≥ 3, = 6,151), ticagrelor was associated with slightly lower risks of ischemic events (2.29% vs. 3.54%, = 0.02) and stroke (0.39% vs. 1.08%, = 0.01) without excessive risk of BARC 3, 5 bleeding events (2.16% vs. 2.11%, P = 0.92) compared to clopidogrel within 12 months after PCI. For patients with low risk (CHADS-VASc < 3, = 10,886), a statistically significant difference was seen in the incidence of overall 12-month BARC 2, 3, 5 bleeding events by P2Y receptor inhibitor (4.00% vs. 3.26%) with a similar incidence of the ischemic events (1.40% vs. 1.52%). Results in the PSM cohort and the adjustment with Cox multivariate analysis were consistent with the main outcomes.
Higher CHADS-VASc scores were associated with a higher incidence of 1-year ischemic events for the patients with ACS after PCI. Compared with clopidogrel, ticagrelor was associated with lower ischemic events within 12 months after PCI without excessive risk of bleeding in high-risk patients but shows poor safety with excess bleeding in low-risk patients.
在现实世界中,替格瑞洛与氯吡格雷相比,对于接受经皮冠状动脉介入治疗(PCI)的非选择性急性冠状动脉综合征(ACS)患者的临床获益仍存在争议。本研究旨在基于CHADS-VASc评分进行风险分层,探讨替格瑞洛与氯吡格雷对PCI术后无房颤或房扑(AF)的ACS患者的影响。
在2016年至2019年期间,北部战区总医院至少植入一枚支架的PCI患者根据CHADS-VASc评分分为低风险或高风险组。评估阿司匹林联合不同P2Y抑制剂(氯吡格雷或替格瑞洛)在不同风险组中12个月缺血事件(心源性死亡、心肌梗死[MI]或卒中)、全因死亡、出血学术研究联盟(BARC)2、3、5级出血、BARC 3、5级出血以及净不良临床事件(NACEs)(全因死亡、MI、卒中或BARC 3、5级出血)的发生率。采用倾向评分匹配(PSM)和Cox多变量分析来平衡各组。
共纳入连续17037例ACS患者。通过约登检验确定的CHADS-VASc评分对缺血事件的最佳截断值为3分。在高风险患者(CHADS-VASc≥3,n = 6151)中,与氯吡格雷相比,替格瑞洛在PCI术后12个月内缺血事件风险略低(2.29%对3.54%,P = 0.02),卒中风险也较低(0.39%对1.08%,P = 0.01),且无BARC 3、5级出血事件的额外风险(2.16%对2.11%,P = 0.92)。对于低风险患者(CHADS-VASc < 3,n = 10886),P2Y受体抑制剂导致的12个月总体BARC 2、3、5级出血事件发生率存在统计学显著差异(4.00%对3.26%),缺血事件发生率相似(1.40%对1.52%)。PSM队列结果及Cox多变量分析调整结果与主要结局一致。
较高的CHADS-VASc评分与PCI术后ACS患者1年缺血事件发生率较高相关。与氯吡格雷相比,替格瑞洛在PCI术后12个月内缺血事件风险较低,高风险患者无出血额外风险,但低风险患者出血过多显示安全性较差。