Department of Medicine, Smt. NHL Municipal Medical College, Ahmedabad, Gujarat, India.
Department of Internal Medicine, Temple University Hospital, Philadelphia, PA, 19140, USA.
BMC Neurol. 2022 Apr 22;22(1):151. doi: 10.1186/s12883-022-02676-4.
The Guillain-Barre Syndrome (GBS), also known as acute idiopathic polyneuritis, is a critical acquired condition associated with preceding nonspecific infection or triggering factors like trauma, surgery, or vaccination. GBS is currently the most frequent cause of acute flaccid paralysis in India. This study evaluates the short-term and in-hospital outcomes in different subtypes of GBS.
A prospective observational study was conducted at V.S. Hospital, Ahmedabad, from September 2015 to December 2017. Patients above the age of 12 were included. Patients having other underlying neurological conditions, as well as immunodeficiency disorders, were excluded. The patients were classified into different subtypes of GBS, and functional outcomes were recorded on admission and discharge according to Hughes Scoring System. All statistical analyses were performed by using SPSS software.
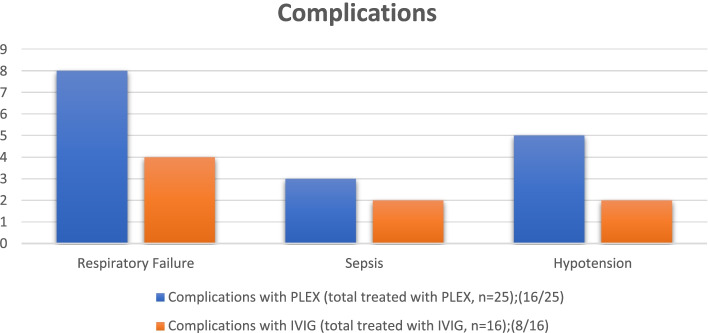
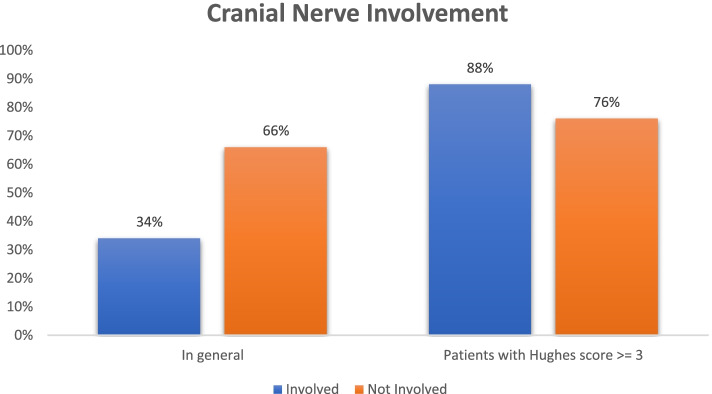
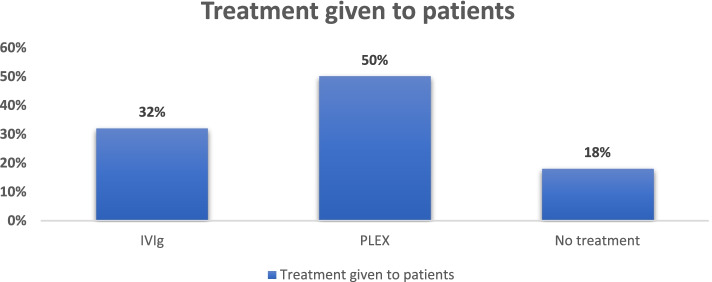
Out of 50 patients, 35 (70%) were males. The mean age was of 37.18 +/- 18.35 years. 25 (50%) patients had a preceding infection. 88% of patients presented with cranial nerve (CN) involvement had a Hughes Score of >/= 3 (p = 0.0087). They had less improvement of Hughes Score on discharge (0.13 +/- 0.04) as compared to the patients without cranial nerve involvement (0.38 +/- 0.08) (p = 0.008). Respiratory involvement was associated with a higher Hughes Score (p = 0.005) on admission. 85% of patients diagnosed with an axonal subtype of GBS had a Hughes Score of >/= 3 (p = 0.06) compared to 74% patients with demyelinating subtype. Axonal subtype required double period (11 +/- 2.34) to show improvement as compared to demyelinating subtype (6 +/- 1.2) (p = 0.020). Irrespective of the subtypes, in two different treatment cohorts (PLEX vs IVIG), there was no difference in short term functional outcomes measured by improvement in the Hughes scores (p = 0.89).
Early cranial nerve and respiratory involvement in patients presenting with GBS are associated with poor outcomes warranting immediate critical care involvement. In our study, amongst all the subtypes, axonal had poor clinical outcomes. Further clinical trials on the Indian subpopulation will help us evaluate the impact of different treatment modalities on this disease.
吉兰-巴雷综合征(GBS),也称为急性特发性多神经炎,是一种与非特异性感染或创伤、手术、疫苗接种等触发因素相关的严重获得性疾病。GBS 是目前印度急性弛缓性麻痹最常见的病因。本研究评估了不同 GBS 亚型的短期和住院结局。
这是一项于 2015 年 9 月至 2017 年 12 月在印度艾哈迈达巴德的 V.S. 医院进行的前瞻性观察性研究。纳入年龄在 12 岁以上的患者。排除有其他潜在神经疾病和免疫功能障碍的患者。根据 Hughes 评分系统,将患者分为不同的 GBS 亚型,并在入院和出院时记录功能结局。所有统计分析均使用 SPSS 软件进行。
在 50 名患者中,35 名(70%)为男性。平均年龄为 37.18 ± 18.35 岁。25 名(50%)患者有前驱感染。88%有颅神经(CN)受累的患者 Hughes 评分>/= 3(p=0.0087)。与无脑神经受累的患者相比,他们在出院时 Hughes 评分的改善程度较低(0.13 ± 0.04 对 0.38 ± 0.08)(p=0.008)。入院时存在呼吸受累与较高的 Hughes 评分相关(p=0.005)。85%诊断为轴索性 GBS 的患者 Hughes 评分>/= 3(p=0.06),而脱髓鞘性 GBS 患者为 74%。轴索性 GBS 患者需要两个周期(11 ± 2.34)才能改善,而脱髓鞘性 GBS 患者需要 6 ± 1.2 个周期(p=0.020)。无论亚型如何,在接受 PLEX 与 IVIG 两种不同治疗方案的患者中,Hughes 评分改善的短期功能结局没有差异(p=0.89)。
GBS 患者早期出现颅神经和呼吸受累与不良结局相关,需要立即进行重症监护治疗。在我们的研究中,在所有亚型中,轴索性 GBS 具有较差的临床结局。在印度人群中进行的进一步临床试验将帮助我们评估不同治疗方式对这种疾病的影响。