Nemitz Lena, Vincke Anna, Michalik Bianca, Engels Svenja, Meyer Luca-Marie, Henke Rolf-Peter, Wawroschek Friedhelm, Winter Alexander
University Hospital for Urology, Klinikum Oldenburg, Department of Human Medicine, School of Medicine and Health Sciences, Carl von Ossietzky University Oldenburg, Oldenburg, Germany.
Institute of Pathology Oldenburg, Oldenburg, Germany.
Front Oncol. 2022 Apr 14;12:850905. doi: 10.3389/fonc.2022.850905. eCollection 2022.
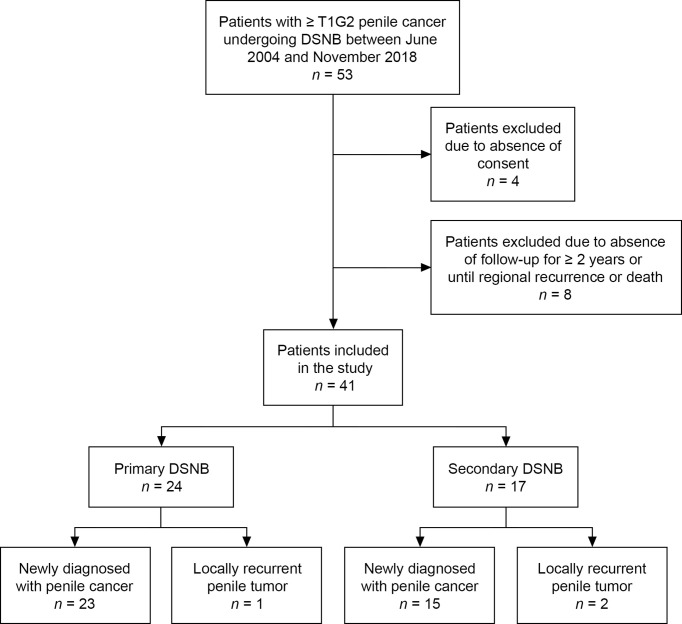
Lymph node (LN) management is critical for survival in patients with penile cancer. However, radical inguinal lymphadenectomy carries a high risk of postoperative complications such as lymphedema, lymphocele, wound infection, and skin necrosis. The European Association of Urology guidelines therefore recommend invasive LN staging by modified inguinal lymphadenectomy or dynamic sentinel node biopsy (DSNB) in clinically node-negative patients (cN0) with intermediate- and high-risk tumors (≥ T1G2). However, the timing of DSNB (simultaneous vs. subsequent to partial or total penile resection) is controversial and the low incidence of penile cancer means that data on the long-term outcomes of DSNB are limited. The present study aimed to analyze the reliability and morbidity of DSNB in patients with penile cancer during long-term follow-up. This retrospective study included 41 patients (76 groins) who underwent radioisotope-guided DSNB simultaneously or secondarily after penile surgery from June 2004 to November 2018. In total, 193 sentinel LNs (SLNs) and 39 non-SLNs were removed. The median number of dissected LNs was 2.5 (interquartile range 2-4). Histopathological analysis showed that five of the 76 groins (6.6%) contained metastases. None of the non-SLNs were tumor-positive. In accordance with the guidelines, all inguinal regions with positive SLNs underwent secondary radical inguinal lymphadenectomy, which revealed three additional metastases in one groin. Regional LN recurrence was detected in three patients (four groins) during a median follow-up of 70 months, including two patients in whom DSNB had been performed secondarily after repetitive penile tumor resections. DSNB-related complications occurred in 15.8% of groins. Most complications were mild (Clavien-Dindo grade I; 50%) or moderate (II; 25%), and invasive intervention was only required in 3.9% of groins (IIIa: = 1; IIIb: = 2). In summary, this study suggests that the current radioisotope-guided DSNB procedure may reduce the complication rate of inguinal lymphadenectomy in patients with cN0 penile cancer. However, DSNB and penile surgery should be performed simultaneously to minimize the false-negative rate. Recent advances, such as new tracers and imaging techniques, may help to reduce the false-negative rate of DSNB further.
淋巴结(LN)管理对于阴茎癌患者的生存至关重要。然而,根治性腹股沟淋巴结清扫术术后并发症的风险很高,如淋巴水肿、淋巴囊肿、伤口感染和皮肤坏死。因此,欧洲泌尿外科学会指南建议,对于临床淋巴结阴性(cN0)的中高危肿瘤(≥T1G2)患者,通过改良腹股沟淋巴结清扫术或动态前哨淋巴结活检(DSNB)进行侵入性LN分期。然而,DSNB的时机(与部分或全阴茎切除同时进行还是在其后进行)存在争议,而且阴茎癌发病率较低,这意味着关于DSNB长期结果的数据有限。本研究旨在分析阴茎癌患者长期随访期间DSNB的可靠性和发病率。这项回顾性研究纳入了2004年6月至2018年11月期间接受放射性同位素引导下DSNB的41例患者(76个腹股沟),这些患者在阴茎手术后同时或二次进行了该检查。总共切除了193个前哨淋巴结(SLN)和39个非SLN。切除淋巴结的中位数为2.5个(四分位间距为2 - 4个)。组织病理学分析显示,76个腹股沟中有5个(6.6%)存在转移。所有非SLN均未发现肿瘤阳性。根据指南,所有SLN阳性的腹股沟区域均接受了二次根治性腹股沟淋巴结清扫术,结果在一个腹股沟中又发现了3处转移。在中位随访70个月期间,3例患者(4个腹股沟)检测到区域LN复发,其中2例患者在反复阴茎肿瘤切除术后二次进行了DSNB。DSNB相关并发症发生在15.8%的腹股沟中。大多数并发症为轻度(Clavien - Dindo分级I级;50%)或中度(II级;25%),仅3.9%的腹股沟需要进行侵入性干预(IIIa级:= 1例;IIIb级:= 2例)。总之,本研究表明,目前放射性同位素引导下的DSNB程序可能会降低cN阴茎癌患者腹股沟淋巴结清扫术的并发症发生率。然而,DSNB和阴茎手术应同时进行,以尽量降低假阴性率。新的示踪剂和成像技术等最新进展可能有助于进一步降低DSNB的假阴性率。