Cuccia Francesco, Rigo Michele, Figlia Vanessa, Giaj-Levra Niccolò, Mazzola Rosario, Nicosia Luca, Ricchetti Francesco, Trapani Giovanna, De Simone Antonio, Gurrera Davide, Naccarato Stefania, Sicignano Gianluisa, Ruggieri Ruggero, Alongi Filippo
Advanced Radiation Oncology Department, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Sacro Cuore Don Calabria Hospital, Negrar di Valpolicella, Italy.
University of Brescia, Brescia, Italy.
Front Oncol. 2022 Apr 13;12:858740. doi: 10.3389/fonc.2022.858740. eCollection 2022.
Prostate re-irradiation is an attractive treatment option in the case of local relapse after previous radiotherapy, either in the definitive or in the post-operative setting. In this scenario, the introduction of MR-linacs may represent a helpful tool to improve the accuracy and precision of the treatment.
This study reports the preliminary data of a cohort of 22 patients treated with 1.5T MR-Linacs for prostate or prostate bed re-irradiation. Toxicity was prospectively assessed and collected according to CTCAE v5.0. Survival endpoints were measured using Kaplan-Meier method.
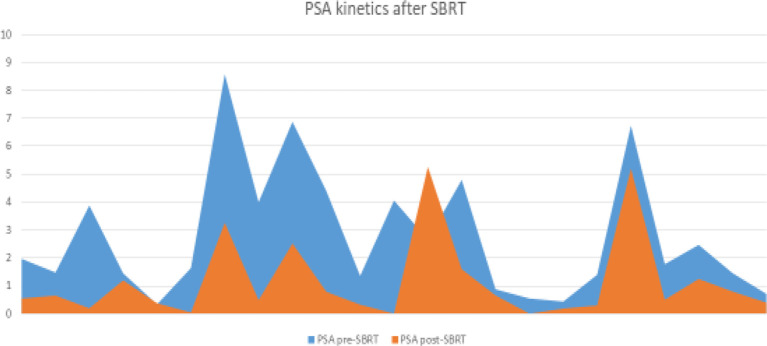
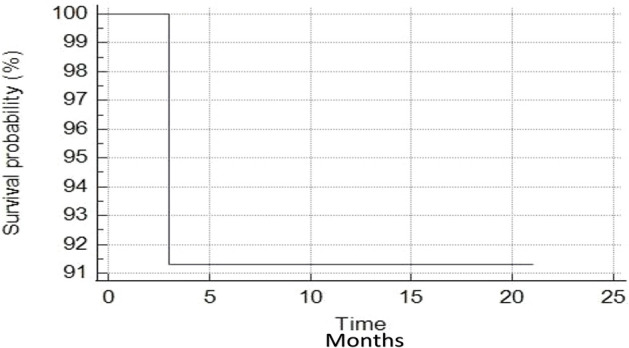
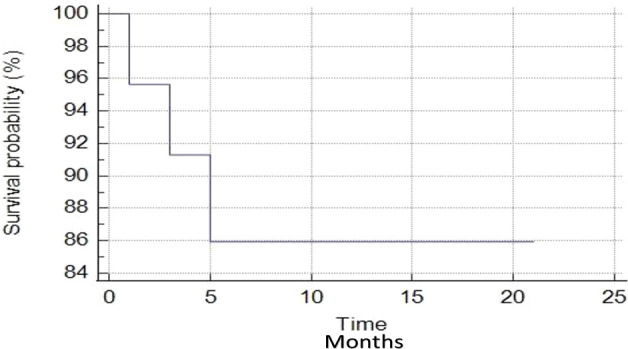
From October 2019 to October 2021, 22 patients received 1.5T MR-guided stereotactic body radiotherapy for prostate or prostate-bed re-irradiation. In 12 cases SBRT was delivered to the prostate, in 10 to the prostate bed. The median time to re-RT was 72 months (range, 12-1460). SBRT was delivered concurrently with ADT in 4 cases. Acute toxicity was: for GU G1 in 11/22 and G2 in 4/22; for GI G1 in 7/22, G2 in 4/22. With a median follow-up of 8 months (3-21), late G1 and G2 GU events were respectively 11/22 and 4/22. Regarding GI toxicity, G1 were 6/22, while G2 3/22. No acute/late G≥3 GI/GU events occurred. All patients are alive. The median PSA-nadir was 0.49 ng/ml (0.08-5.26 ng/ml), for 1-year BRFS and DPFS rates of 85.9%. Twenty patients remained free from ADT with 1-year ADT-free survival rates of 91.3%.
Our experience supports the use of MR-linacs for prostate or prostate bed re-irradiation as a feasible and safe treatment option with minimal toxicity and encouraging results in terms of clinical outcomes.
对于先前接受过确定性放疗或术后放疗后出现局部复发的情况,前列腺再照射是一种有吸引力的治疗选择。在这种情况下,磁共振直线加速器(MR-linacs)的引入可能是提高治疗准确性和精确性的有用工具。
本研究报告了一组22例接受1.5T MR直线加速器进行前列腺或前列腺床再照射患者的初步数据。根据CTCAE v5.0对毒性进行前瞻性评估和收集。使用Kaplan-Meier方法测量生存终点。
从2019年10月至2021年10月,22例患者接受了1.5T磁共振引导的立体定向体部放疗用于前列腺或前列腺床再照射。12例患者对前列腺进行了立体定向体部放疗(SBRT),10例对前列腺床进行了SBRT。再放疗的中位时间为72个月(范围12 - 1460个月)。4例患者SBRT与雄激素剥夺治疗(ADT)同时进行。急性毒性反应为:泌尿系统(GU)方面,11/22为1级,4/22为2级;胃肠道(GI)方面,7/22为1级,4/22为2级。中位随访时间为8个月(3 - 21个月),晚期1级和2级泌尿系统事件分别为11/22和4/22。关于胃肠道毒性,1级为6/22,2级为3/22。未发生急性/晚期3级及以上胃肠道/泌尿系统事件。所有患者均存活。PSA最低点的中位数为0.49 ng/ml(0.08 - 5.26 ng/ml),1年生化无复发生存率(BRFS)和远处无复发生存率(DPFS)为85.9%。20例患者维持无ADT状态,1年无ADT生存率为91.3%。
我们的经验支持使用MR直线加速器进行前列腺或前列腺床再照射,作为一种可行且安全的治疗选择,毒性最小,临床结果令人鼓舞。