Lee Yung-Tsai, Yin Wei-Hsian, Tsao Tien-Ping, Lee Kuo-Chen, Hsiung Ming-Chon, Tzeng Yun-Hsuan, Wei Jeng
Heart Center, Cheng Hsin General Hospital, Taipei, Taiwan.
Institute of Microbiology and Immunology, National Yang Ming Chiao Tung University, Taipei, Taiwan.
Front Cardiovasc Med. 2022 Apr 13;9:767906. doi: 10.3389/fcvm.2022.767906. eCollection 2022.
Current guidelines recommend that transcatheter aortic valve replacement (TAVR) for bicuspid aortic valve (BAV) with aortic stenosis (AS) should only be performed in selected patients. However, we consider it even more crucial to identify what the really important factors are while determining long-term outcomes in patients with BAV undergoing TAVR, which is precisely the aim of this study.
We retrospectively evaluated consecutive patients who underwent TAVR with balloon-expandable Sapien XT or Sapien 3 valves (Edwards Lifesciences, Irvine, CA) for the treatment of severe bicuspid AS. The primary end points were major adverse cardiac and cerebral events (MACCE), that is, mortality, non-fatal myocardial infarction (MI), disabling stroke, valve failure needing reintervention, or clinically relevant valve thrombosis during follow-up.
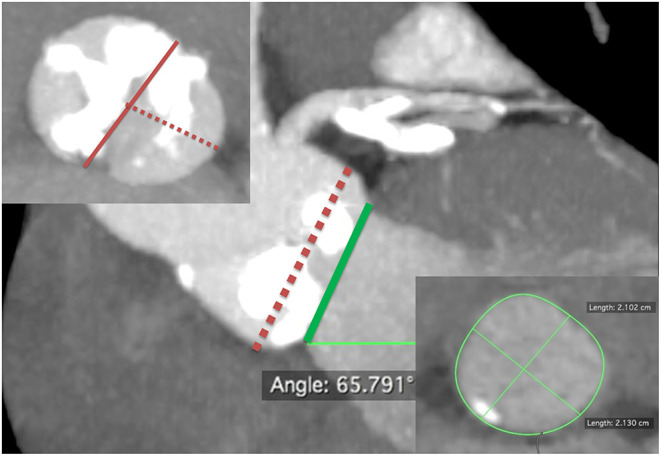
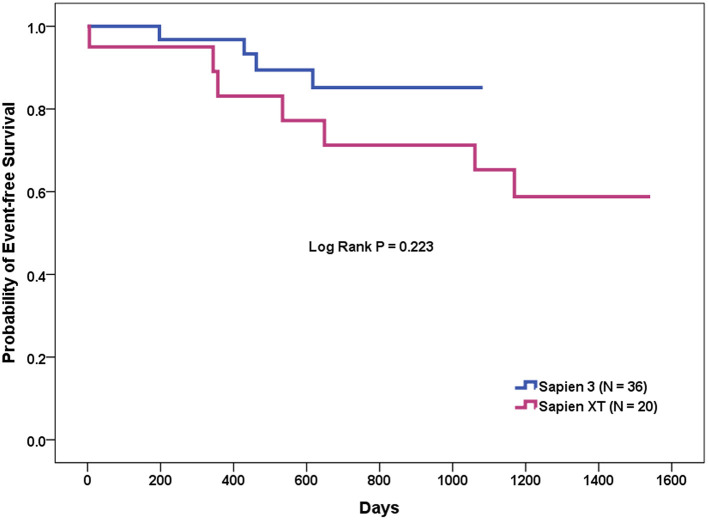
A total of 56 patients who underwent TAVR with Sapien XT ( = 20) or Sapien 3 ( = 36) were included. The device and procedural success rates were similar between the two TAVR valves; however, the newer-generation Sapien 3 yielded a trend toward better long-term clinical outcomes than the early-generation Sapien XT did (MACCE rates 35 vs. 11%, = 0.071). In the multivariate Cox proportional hazards analyses, the presence of calcified raphe > 4 mm was the only independent predictor of long-term MACCE (hazard ratio: 6.76; 95% confidence interval: 1.21-37.67, = 0.029).
TAVR performed by a skilled heart team, while using newer-generation balloon-expandable Sapien 3 valve, may yield better long-term clinical outcomes compared to TAVR using early-generation Sapien XT valve. Moreover, the presence of calcified raphe >4 mm is an independent determinant of adverse clinical outcomes.
当前指南建议,经导管主动脉瓣置换术(TAVR)仅适用于特定患者的二叶式主动脉瓣(BAV)伴主动脉狭窄(AS)。然而,我们认为,在确定接受TAVR的BAV患者的长期预后时,识别真正重要的因素更为关键,而这正是本研究的目的。
我们回顾性评估了连续接受球囊扩张式Sapien XT或Sapien 3瓣膜(爱德华生命科学公司,加利福尼亚州尔湾)TAVR治疗严重二叶式AS的患者。主要终点是主要不良心脑血管事件(MACCE),即随访期间的死亡率、非致命性心肌梗死(MI)、致残性中风、需要再次干预的瓣膜功能衰竭或临床相关的瓣膜血栓形成。
共有56例接受Sapien XT(n = 20)或Sapien 3(n = 36)TAVR的患者纳入研究。两种TAVR瓣膜的器械成功率和手术成功率相似;然而,新一代Sapien 3瓣膜的长期临床预后趋势优于早期的Sapien XT瓣膜(MACCE发生率分别为35%和11%,P = 0.071)。在多变量Cox比例风险分析中,钙化嵴>4 mm是长期MACCE的唯一独立预测因素(风险比:6.76;95%置信区间:1.21 - 37.67,P = 0.029)。
与使用早期Sapien XT瓣膜的TAVR相比,由经验丰富的心脏团队进行的TAVR,同时使用新一代球囊扩张式Sapien 3瓣膜,可能会产生更好的长期临床预后。此外,钙化嵴>4 mm是不良临床预后的独立决定因素。