Tran Anh Dam, Hong Angela M, Nguyen Mai T H, Fogarty Gerald, Steel Victoria, Paton Elizabeth, Morton Rachael L
National Drug and Alcohol Research Centre, UNSW, Sydney, Australia.
NHMRC Clinical Trials Centre, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia.
Pharmacoecon Open. 2022 Jul;6(4):587-594. doi: 10.1007/s41669-022-00332-8. Epub 2022 May 5.
We aimed to compare Australian health system costs at 12 months for adjuvant whole-brain radiotherapy (WBRT) treatment after stereotactic radiosurgery (SRS) and/or surgery versus observation among adults with one to three melanoma brain metastases. We hypothesized that treatment with adjuvant WBRT and subsequent healthcare would be more expensive than SRS/surgery alone.
The analysis was conducted alongside a multicentre, randomized phase III trial. A bespoke cost questionnaire was used to measure healthcare use, including hospitalizations, specialist and primary care visits, imaging, and medicines over 12 months. Mean per-patient costs were calculated based on the quantity of resources used and unit costs, reported in Australian dollars ($AU), year 2018 values. Skewness of cost data was determined using normality tests and censor-adjusted costs reported using the Kaplan-Meier sample average method. The analysis of difference in mean costs at each 2-month time point and at 12 months was performed and checked using Kruskal-Wallis, generalized linear models with gamma distribution and log link, modified Park test, ordinary least squares, and non-parametric bootstrapping.
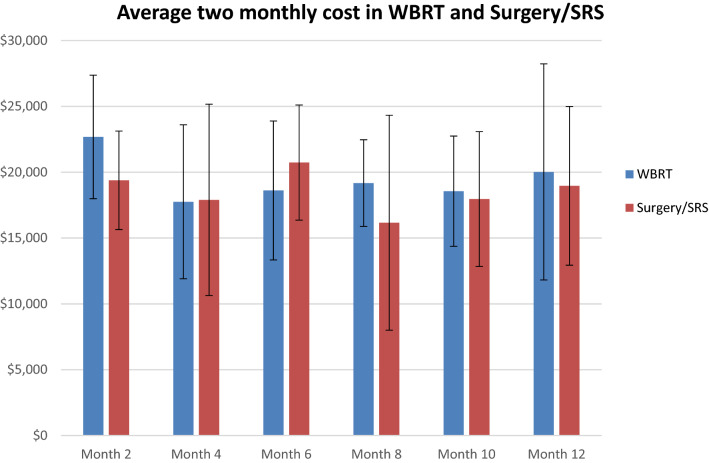
In total, 89 patients with similar characteristics at baseline were included in the cost analysis (n = 43 WBRT; n = 46 observation). Hospitalization cost was the main cost, ranging from 63 to 89% of total healthcare costs. The unadjusted 12-monthly cost for WBRT was $AU71,138 ± standard deviation 41,475 and for observation $AU69,848 ± 33,233; p = 0.7426. The censor-adjusted 12-monthly cost for WBRT was $AU90,277 ± 36,274 and $AU82,080 ± 34,411 for observation. There was no significant difference in 2-monthly costs between groups (p > 0.30 for all models).
Most costs were related to inpatient hospitalizations associated with disease recurrence. Adding WBRT after local SRS/surgery for patients with one to three melanoma brain metastases did not significantly increase health system costs during the first 12 months.
ACTRN12607000512426, prospectively registered 14 September 2007.
我们旨在比较立体定向放射外科手术(SRS)和/或手术后辅助全脑放疗(WBRT)与观察等待对一至三个黑色素瘤脑转移瘤成年患者12个月时澳大利亚卫生系统成本的影响。我们假设辅助WBRT治疗及后续医疗保健费用会高于单纯SRS/手术。
该分析与一项多中心、随机III期试验同时进行。使用定制的成本问卷来衡量医疗保健使用情况,包括12个月内的住院、专科和初级保健就诊、影像学检查及药物使用。根据使用的资源数量和单位成本计算每位患者的平均成本,以2018年澳元($AU)为单位。使用正态性检验确定成本数据的偏度,并使用Kaplan-Meier样本平均法报告经审查调整后的成本。在每个2个月时间点和12个月时对平均成本差异进行分析,并使用Kruskal-Wallis检验、具有伽马分布和对数链接的广义线性模型、修正的Park检验、普通最小二乘法和非参数自抽样法进行检查。
成本分析共纳入89例基线特征相似患者(WBRT组43例;观察等待组46例)。住院成本是主要成本,占总医疗保健成本的63%至89%。WBRT组未经调整的12个月成本为71,138澳元±标准差41,475,观察等待组为69,848澳元±33,233;p = 0.7426。WBRT组经审查调整的12个月成本为90,277澳元±36,274,观察等待组为82,080澳元±34,411。两组间2个月成本无显著差异(所有模型p>0.30)。
大部分成本与疾病复发相关的住院治疗有关。对于一至三个黑色素瘤脑转移瘤患者,在局部SRS/手术后加用WBRT在最初12个月内未显著增加卫生系统成本。
ACTRN12607000512426,2007年9月14日前瞻性注册。