Section of Obstetrics and Gynaecology, Clinical Sciences, The Queen's Medical Research Institute, The University of Edinburgh, Edinburgh, UK.
Reprod Fertil. 2022 Apr 5;3(2):R66-R90. doi: 10.1530/RAF-21-0095. eCollection 2022 Apr 1.
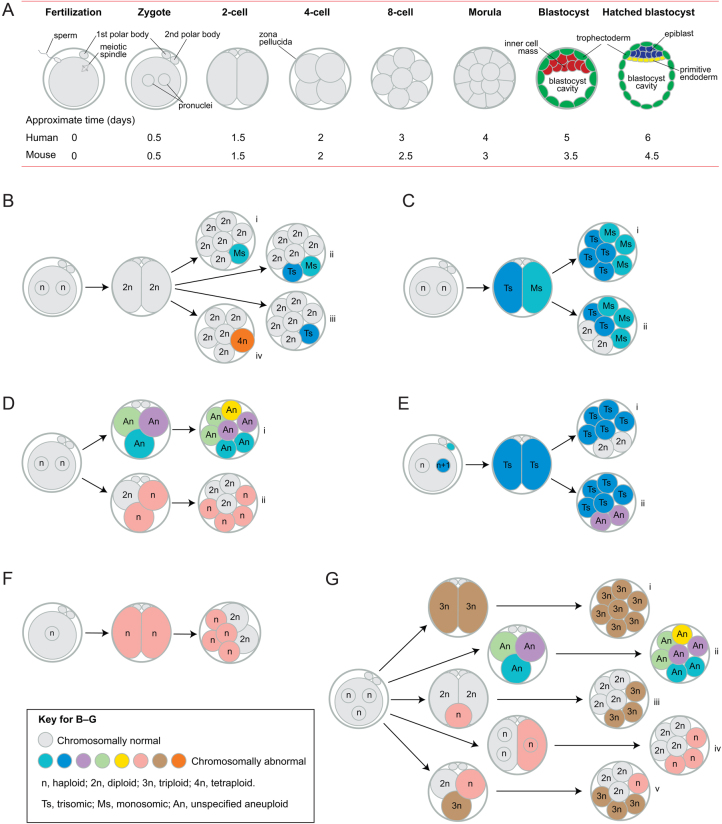
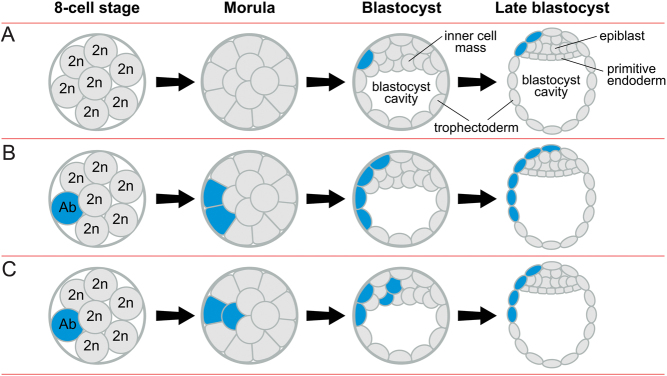
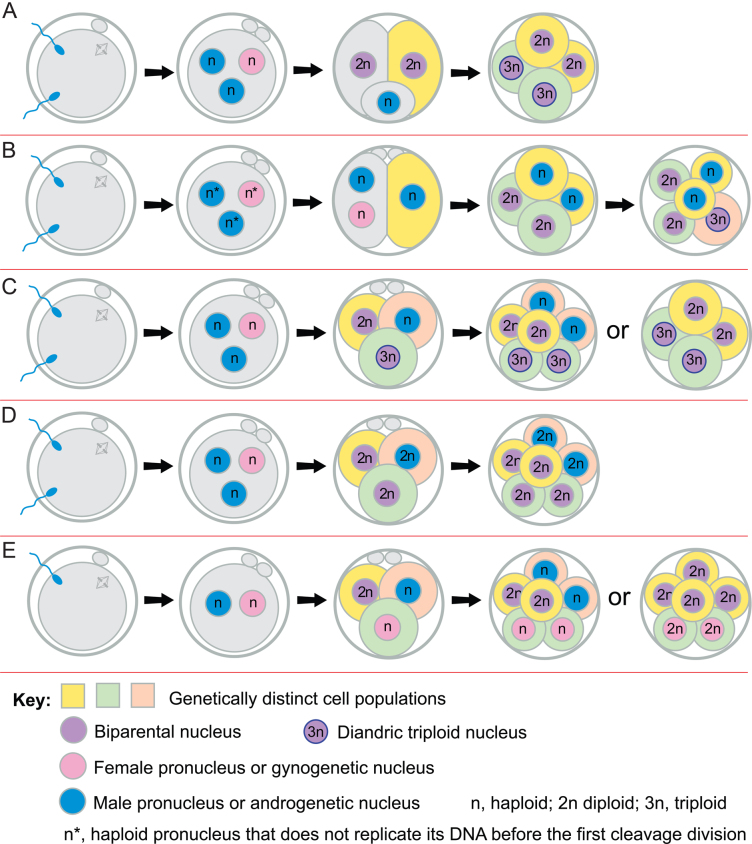
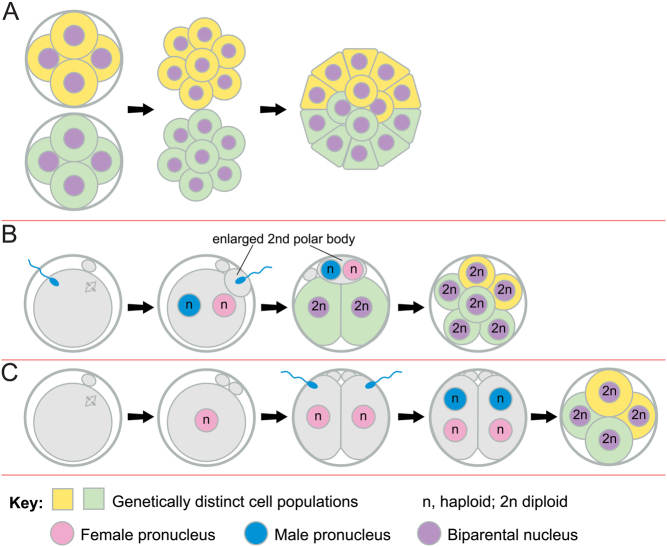
Some human preimplantation embryos are chromosomally mosaic. For technical reasons, estimates of the overall frequency vary widely from <15 to >90% and the true frequency remains unknown. Aneuploid/diploid and aneuploid/aneuploid mosaics typically arise during early cleavage stages before the embryonic genome is fully activated and when cell cycle checkpoints are not operating normally. Other mosaics include chaotic aneuploid mosaics and mixoploids, some of which arise by abnormal chromosome segregation at the first cleavage division. Chimaeras are similar to mosaics, in having two genetically distinct cell populations, but they arise from more than one zygote and occur less often. After implantation, the frequency of mosaic embryos declines to about 2% and most are trisomic/diploid mosaics, with trisomic cells confined to the placenta. Thus, few babies are born with chromosomal mosaicism. This review discusses the origin of different types of chromosomal mosaics and chimaeras; their fate and the relationship between preimplantation chromosomal mosaicism and confined placental mosaicism in human conceptuses and animal models. Abnormal cells in mosaic embryos may be depleted by cell death, other types of cell selection or cell correction but the most severely affected mosaic embryos probably die. Trisomic cells could become restricted to placental lineages if cell selection or correction is less effective in placental lineages and/or they are preferentially allocated to a placental lineage. However, the relationship between preimplantation mosaicism and confined placental mosaicism may be complex because the specific chromosome(s) involved will influence whether chromosomally abnormal cells survive predominately in the placental trophoblast and/or placental mesenchyme.
Human cells normally have 23 pairs of chromosomes, which carry the genes. During the first few days of development, some human embryos are chromosomal mosaics. These mosaic embryos have both normal cells and cells with an abnormal number of chromosomes, which arise from the same fertilised egg. (More rarely, the different cell populations arise from more than one fertilised egg and these embryos are called chimaeras.) If chromosomally abnormal cells survive to term, they could cause birth defects. However, few abnormal cells survive and those that do are usually confined to the placenta, where they are less likely to cause harm. It is not yet understood how this restriction occurs but the type of chromosomal abnormality influences which placental tissues are affected. This review discusses the origin of different types of chromosomally abnormal cells, their fate and how they might become confined to the placenta in humans and animal models.
一些人类胚胎在植入前存在染色体镶嵌现象。由于技术原因,整体镶嵌频率的估计值差异很大,从<15%到>90%不等,真实频率仍不清楚。非整倍体/整倍体和非整倍体/非整倍体镶嵌体通常在胚胎基因组完全激活之前和细胞周期检查点不能正常工作的早期卵裂阶段出现。其他镶嵌体包括混沌非整倍体镶嵌体和混倍体,其中一些是由于第一次卵裂分裂时染色体异常分离而产生的。嵌合体与镶嵌体相似,具有两个遗传上不同的细胞群体,但它们来自不止一个受精卵,发生的频率较低。植入后,镶嵌胚胎的频率下降到约 2%,大多数为三体/二倍体镶嵌体,三体细胞局限于胎盘。因此,很少有婴儿出生时带有染色体镶嵌现象。这篇综述讨论了不同类型的染色体镶嵌体和嵌合体的起源;它们的命运以及人类胚胎和动物模型中植入前染色体镶嵌体和局限于胎盘的镶嵌体之间的关系。镶嵌胚胎中的异常细胞可能会通过细胞死亡、其他类型的细胞选择或细胞校正而耗尽,但受影响最严重的镶嵌胚胎可能会死亡。如果胎盘谱系中的细胞选择或校正效果较差,或者三体细胞优先分配到胎盘谱系中,那么三体细胞可能会局限于胎盘谱系。然而,植入前镶嵌体和局限于胎盘的镶嵌体之间的关系可能很复杂,因为涉及的特定染色体将影响染色体异常细胞主要存活于胎盘滋养层和/或胎盘间质中。
人类细胞通常有 23 对染色体,携带基因。在发育的头几天,一些人类胚胎是染色体镶嵌体。这些镶嵌胚胎既有正常细胞,也有染色体数目异常的细胞,它们来自同一个受精卵。(更罕见的是,不同的细胞群体来自不止一个受精卵,这些胚胎被称为嵌合体。)如果染色体异常细胞存活到足月,它们可能导致出生缺陷。然而,很少有异常细胞存活下来,那些存活下来的异常细胞通常局限于胎盘,在那里它们不太可能造成伤害。目前还不清楚这种限制是如何发生的,但染色体异常的类型会影响受影响的胎盘组织类型。这篇综述讨论了不同类型的染色体异常细胞的起源、它们的命运以及它们如何在人类和动物模型中局限于胎盘。