Department of Medicine, Cedars-Sinai Medical Center, Los Angeles, California, USA.
Cedars-Sinai Medical Center, Los Angeles, California, USA.
Hepatol Commun. 2022 Sep;6(9):2253-2261. doi: 10.1002/hep4.1981. Epub 2022 May 9.
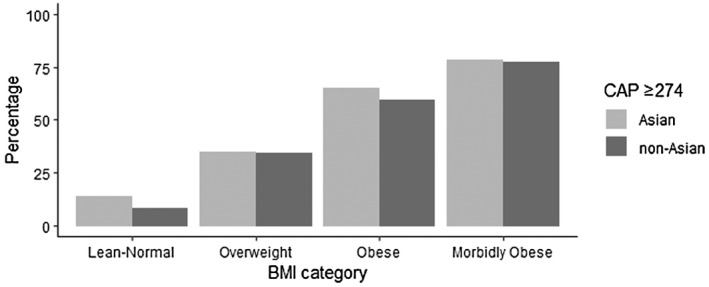
Studies have examined nonalcoholic fatty liver disease (NAFLD) prevalence and severity in Asians; however, this is not well understood in Asian Americans (both East and South Asian Americans) as few studies have analyzed this population. We aimed to describe characteristics, prevalence of NAFLD, and its severity in Asian Americans in the National Health and Nutrition Examination Surveys (NHANES) from 2017 to 2018. Respondents 18 years and older with interview, laboratory testing, and transient elastography data were included. Other causes of liver disease were excluded. Controlled attenuation parameter (CAP) cutoff ≥ 274 dB/m, as published in the literature, defined NAFLD. Sensitivity analysis for CAP cutoffs ≥ 248 and ≥302 dB/m were performed. We found that 450 out of 3639 respondents were Asian Americans, and prevalence using CAP ≥ 274 dB/m was 43.23%. Using sensitivity analysis cutoffs of CAP ≥ 248 dB/m and CAP ≥ 302 dB/m, the prevalence was 57.38% and 28.03%, respectively. Compared with non-Asian Americans with NAFLD, Asian Americans with NAFLD had significantly lower body mass index (BMI) and less prevalent smoking history. Comorbidities, such as prediabetes, diabetes, and hypertension, were not significantly different between Asian and non-Asian Americans with NAFLD. Compared to non-Asian Americans with NAFLD, Asian Americans with NAFLD exhibited higher aminotransferases and triglycerides. Fibrosis assessed by transient elastography was not significantly different between Asian and non-Asian Americans with NAFLD. Despite decreased prevalence of BMI ≥ 30 kg/m , Asian Americans experienced similar NAFLD prevalence with increased hepatocellular injury and triglyceridemia compared to non-Asian Americans. Fibrosis stages were similar to non-Asian Americans.
研究已经检查了非酒精性脂肪性肝病 (NAFLD) 在亚洲人群中的流行率和严重程度;然而,由于很少有研究分析过亚裔美国人(包括东亚裔和南亚裔美国人),因此对此人群的了解并不充分。我们旨在描述 2017 年至 2018 年在国家健康和营养检查调查 (NHANES) 中亚裔美国人的特征、NAFLD 的流行率及其严重程度。纳入了年龄在 18 岁及以上且有访谈、实验室检测和瞬时弹性成像数据的受访者。排除了其他原因引起的肝病。根据文献报道,受控衰减参数 (CAP) 截断值≥274dB/m 定义为 NAFLD。对 CAP 截断值≥248 和≥302dB/m 进行了敏感性分析。我们发现,在 3639 名受访者中有 450 名为亚裔美国人,使用 CAP≥274dB/m 的患病率为 43.23%。使用 CAP≥248dB/m 和 CAP≥302dB/m 的敏感性分析截断值,患病率分别为 57.38%和 28.03%。与患有 NAFLD 的非亚裔美国人相比,患有 NAFLD 的亚裔美国人的体重指数 (BMI) 明显较低,且吸烟史的患病率较低。在患有 NAFLD 的亚裔和非亚裔美国人中,合并症(如糖尿病前期、糖尿病和高血压)没有显著差异。与患有 NAFLD 的非亚裔美国人相比,患有 NAFLD 的亚裔美国人的转氨酶和甘油三酯水平更高。通过瞬时弹性成像评估的纤维化程度在患有 NAFLD 的亚裔和非亚裔美国人之间没有显著差异。尽管 BMI≥30kg/m 的患病率降低,但与非亚裔美国人相比,亚裔美国人的 NAFLD 患病率相似,但肝细胞损伤和甘油三酯水平升高。纤维化分期与非亚裔美国人相似。