Shah Deesha, Umar Zaryab, Ilyas Usman, Nso Nso, Zirkiyeva Milana, Rizzo Vincent
Internal Medicine, Icahn School of Medicine at Mount Sinai, Queens Hospital Center, New York City, USA.
Cureus. 2022 Apr 7;14(4):e23912. doi: 10.7759/cureus.23912. eCollection 2022 Apr.
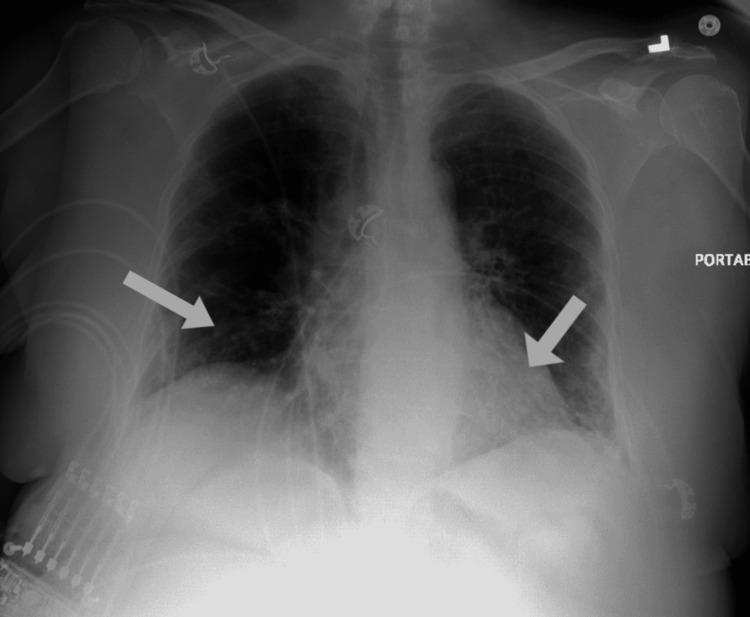
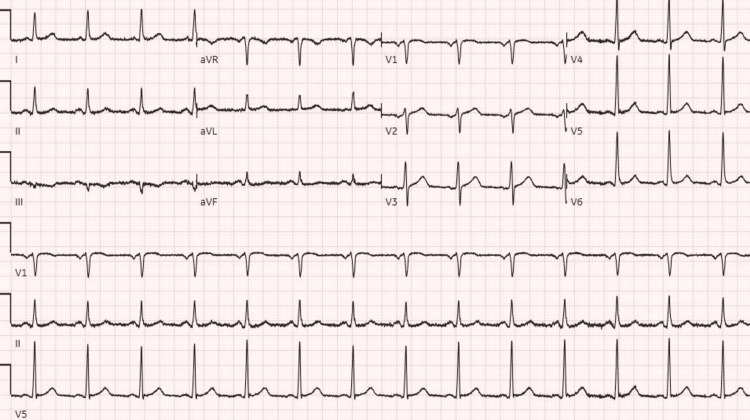
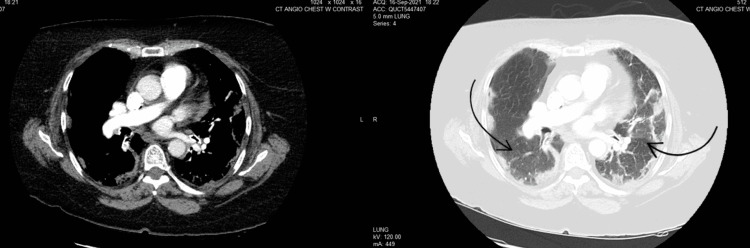
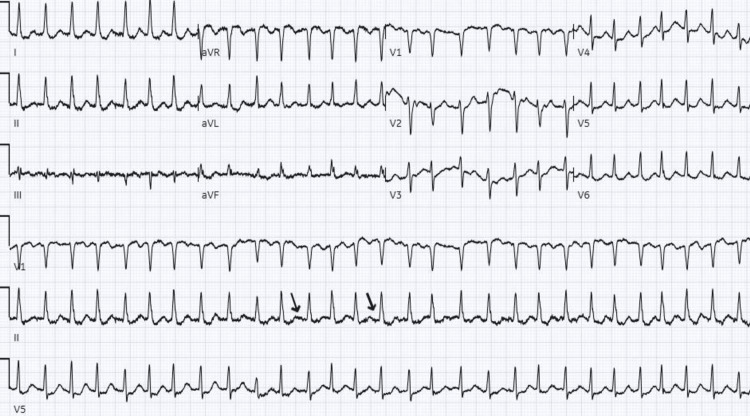
Since the beginning of the coronavirus disease 2019 (COVID-19) pandemic, many cases of arrhythmias have been reported in patients with COVID-19 infection. We present the case of a 66-year-old female with no known cardiovascular history who presented with worsening shortness of breath and productive cough and tested positive for COVID-19 infection in the ED. The patient had a recent hospitalization for COVID-19 infection during which she was treated with dexamethasone and remdesivir therapy and her course remained uncomplicated at that time. Following this, she developed worsening shortness of breath at home for which she presented to the ED. During this hospitalization, she was treated with dexamethasone, remdesivir, and supplemental oxygen. On day six of hospitalization, the patient became tachycardic and had palpitations. Cardiac monitor and EKG showed evidence of new-onset atrial fibrillation (NOAF). Initially patient received metoprolol and diltiazem, both of which failed to achieve adequate rate control. Following this, the patient was started on carvedilol 30 mg every six hours, which attained good rate control. Her CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74, and sex category) score was 4 for which she was started on apixaban 5mg twice daily. The patient was discharged on the same medications. Despite increasing reported incidences of NOAF in COVID-19 infection, only little is known about the optimal management strategies and possible etiopathology. The aim of our review is to highlight the possible mechanisms triggering atrial fibrillation in COVID-19 infection and go over the management strategies while reviewing the available literature.
自2019冠状病毒病(COVID-19)大流行开始以来,已有许多COVID-19感染患者出现心律失常的病例报告。我们报告一例66岁女性病例,该患者无已知心血管病史,因呼吸急促加重和咳痰前来急诊科就诊,COVID-19感染检测呈阳性。该患者近期因COVID-19感染住院,期间接受了地塞米松和瑞德西韦治疗,当时病情未出现并发症。此后,她在家中呼吸急促加重,遂前往急诊科就诊。此次住院期间,她接受了地塞米松、瑞德西韦和补充氧气治疗。住院第六天,患者出现心动过速和心悸。心脏监护仪和心电图显示新发房颤(NOAF)。起初,患者接受了美托洛尔和地尔硫䓬治疗,但均未能实现充分的心率控制。此后,患者开始每6小时服用30毫克卡维地洛,心率得到了良好控制。她的CHA2DS2-VASc(充血性心力衰竭、高血压、年龄≥75岁(加倍)、糖尿病、中风(加倍)、血管疾病、年龄65至74岁以及性别分类)评分为4分,因此开始每天两次服用5毫克阿哌沙班。患者出院时服用相同药物。尽管COVID-19感染中NOAF的报告发病率不断增加,但对于最佳管理策略和可能的病因病理了解甚少。我们综述的目的是在回顾现有文献的同时,强调COVID-19感染中引发房颤的可能机制,并探讨管理策略。