Division of Hematology, Mayo Clinic, Rochester, MN.
Department of Internal Medicine, Mayo Clinic, Rochester, MN.
Blood Adv. 2023 Feb 14;7(3):340-350. doi: 10.1182/bloodadvances.2021006416.
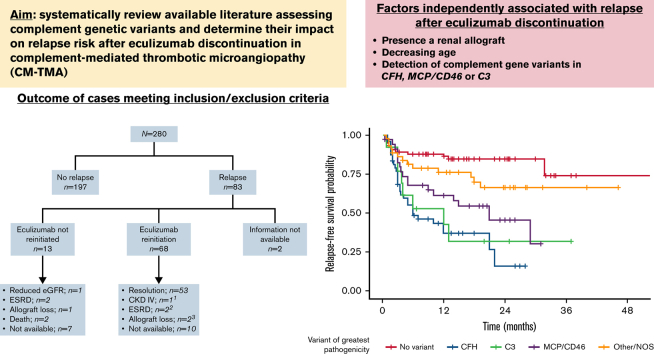
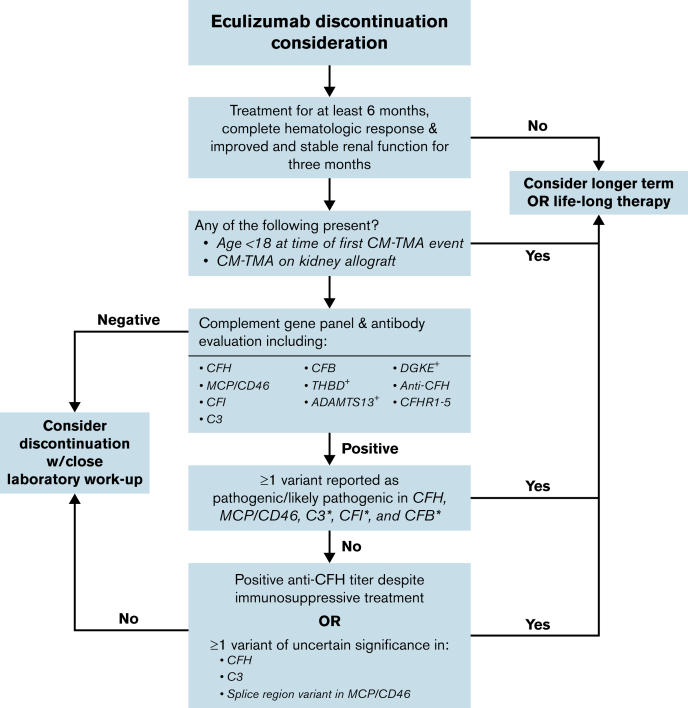
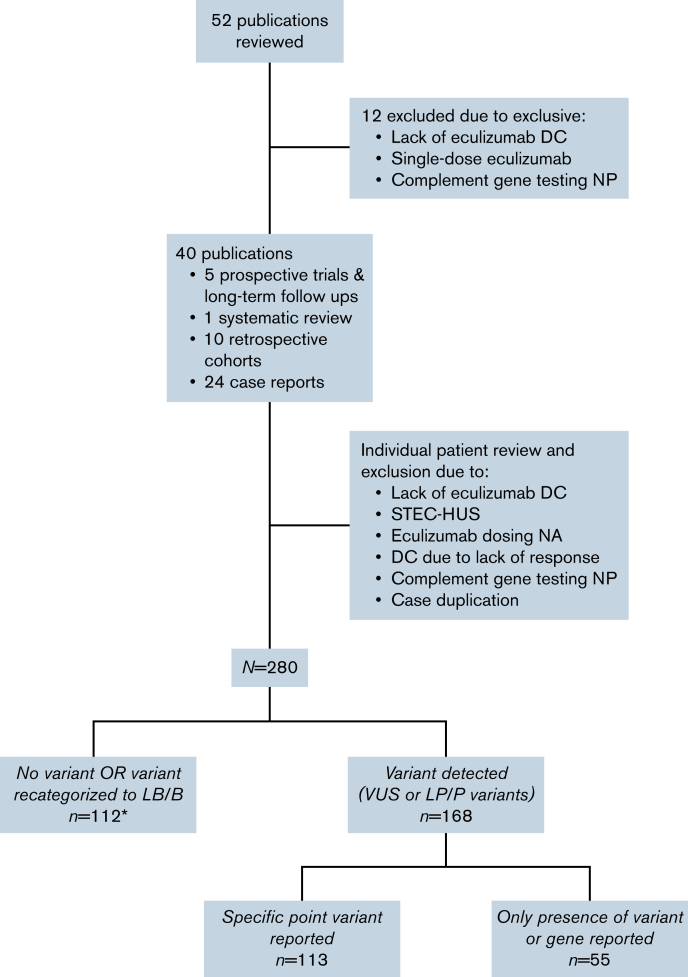
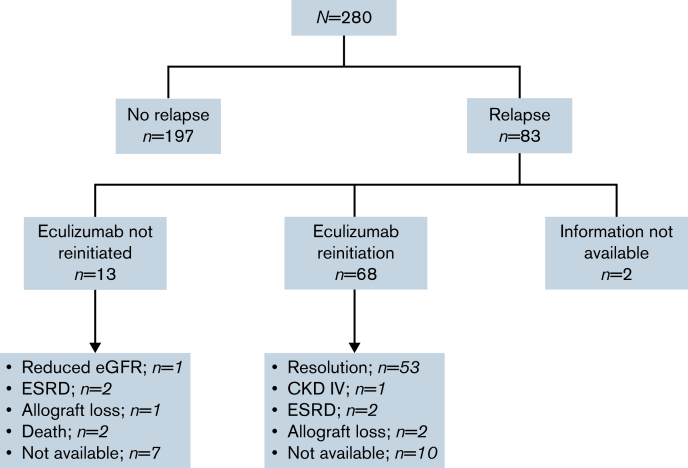
Eculizumab is effective for complement-mediated thrombotic microangiopathy (CM-TMA), also known as atypical hemolytic uremic syndrome. Although lifelong therapy had been suggested, discontinuation does not universally lead to relapse. Comprehensive data evaluating risk factors for recurrence following discontinuation are limited. Our aim was to systematically review available literature assessing the role of complement genetic variants in this setting. Reports on CM-TMA and eculizumab withdrawal published before 1 January 2021, were included. Key reasons for patient exclusion were no follow-up after drug withdrawal and patients lacking complement genetic testing. Two-hundred eighty patients from 40 publications were included. Median age was 28 years, and 25 patients had a known history of renal transplant. Complement genetic variants were identified in 60%, most commonly in CFH (n = 59) and MCP/CD46 (n = 38). Of patients with a complement gene variant, 51.3% had ≥1 likely pathogenic/pathogenic variant whereas the remaining had variants of uncertain significance (VUS). Overall relapse rate after therapy discontinuation was 29.6%. Relapse rate was highest among patients with CFH variants and MCP/CD46 variants in canonical splice regions. VUS (P < .001) and likely pathogenic/pathogenic variants (P < .001) were associated with increased relapse. Presence of a renal allograft (P = .009); decreasing age (P = .029); and detection of variants in CFH (P < .001), MCP/CD46 (P < .001), or C3 (P < .001) were all independently associated with relapse after eculizumab discontinuation. Eculizumab discontinuation is appropriate in specific patients with CM-TMA. Caution should be exerted when attempting such a strategy in patients with high risk of recurrence, including a subgroup of patients with MCP/CD46 variants.
依库珠单抗对补体介导的血栓性微血管病(CM-TMA),也称为非典型溶血尿毒综合征,有效。尽管曾建议终身治疗,但停药并不普遍导致复发。关于停药后复发风险因素的综合数据有限。我们的目的是系统地回顾评估补体遗传变异在这种情况下的作用的现有文献。纳入截止至 2021 年 1 月 1 日之前发表的关于 CM-TMA 和依库珠单抗停药的报告。排除患者的主要原因是停药后无随访和患者缺乏补体遗传检测。40 项研究中有 280 名患者纳入。中位年龄为 28 岁,25 名患者有肾移植史。60%的患者确定了补体遗传变异,最常见的是 CFH(n=59)和 MCP/CD46(n=38)。在有补体基因突变的患者中,51.3%有≥1 个可能致病性/致病性变异,其余患者有意义未明的变异(VUS)。停药后总复发率为 29.6%。CFH 变异和经典剪接区 MCP/CD46 变异的患者复发率最高。VUS(P<0.001)和可能致病性/致病性变异(P<0.001)与复发增加相关。存在肾移植(P=0.009);年龄减小(P=0.029);CFH(P<0.001)、MCP/CD46(P<0.001)或 C3(P<0.001)检测到变异,均与依库珠单抗停药后复发独立相关。在特定的 CM-TMA 患者中,停止使用依库珠单抗是合适的。在试图采取这种策略时,应谨慎对待高复发风险的患者,包括 MCP/CD46 变异的亚组患者。