Département d'Anesthésie Réanimation, Centre Hospitalier Lyon Sud.
REA-REZO Infections et Antibiorésistance en Réanimation, Hôpital Henry Gabrielle.
Am J Respir Crit Care Med. 2022 Jul 15;206(2):161-169. doi: 10.1164/rccm.202202-0357OC.
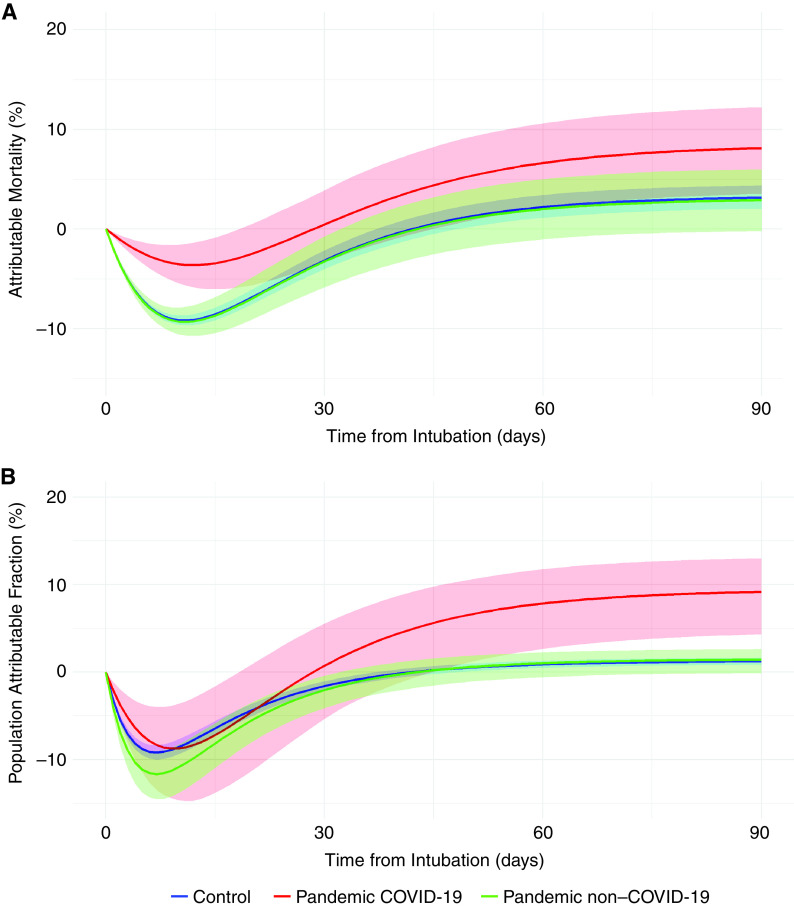
Patients with a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection are at higher risk of ventilator-associated pneumonia (VAP) and may have an increased attributable mortality (increased or decreased risk of death if VAP occurs in a patient) and attributable fraction (proportion of deaths that are attributable to an exposure) of VAP-related mortality compared with subjects without coronavirus disease (COVID-19). Estimation of the attributable mortality of the VAP among patients with COVID-19. Using the REA-REZO surveillance network, three groups of adult medical ICU patients were computed: control group (patients admitted between 2016 and 2019; prepandemic patients), pandemic COVID-19 group (PandeCOV), and pandemic non-COVID-19 group (PandeCOV) admitted during 2020. The primary outcome was the estimation of attributable mortality and attributable fraction related to VAP in these patients. Using multistate modeling with causal inference, the outcomes related to VAP were also evaluated. A total of 64,816 patients were included in the control group, 7,442 in the PandeCOV group, and 1,687 in the PandeCOV group. The incidence of VAP was 14.2 (95% confidence interval [CI], 13.9 to 14.6), 18.3 (95% CI, 17.3 to 19.4), and 31.9 (95% CI, 29.8 to 34.2) per 1,000 ventilation-days in each group, respectively. Attributable mortality at 90 days was 3.15% (95%, CI, 2.04% to 3.43%), 2.91% (95% CI, -0.21% to 5.02%), and 8.13% (95% CI, 3.54% to 12.24%), and attributable fraction of mortality at 90 days was 1.22% (95% CI, 0.83 to 1.63), 1.42% (95% CI, -0.11% to 2.61%), and 9.17% (95% CI, 3.54% to 12.24%) for the control, PandeCOV, and PandeCOV groups, respectively. Except for the higher risk of developing VAP, the PandeCOV group shared similar VAP characteristics with the control group. PandeCOV patients were at lower risk of death without VAP (hazard ratio, 0.62; 95% CI, 0.52 to 0.74) than the control group. VAP-attributable mortality was higher for patients with COVID-19, with more than 9% of the overall mortality related to VAP.
患有严重急性呼吸系统综合症冠状病毒 2 (SARS-CoV-2) 感染的患者发生呼吸机相关性肺炎 (VAP) 的风险较高,与无冠状病毒病 (COVID-19) 的患者相比,VAP 相关死亡率的归因死亡率 (如果 VAP 发生在患者中,死亡率的增加或减少风险) 和归因分数 (归因于暴露的死亡比例) 可能增加。 COVID-19 患者中 VAP 的归因死亡率估计。 使用 REA-REZO 监测网络,计算了三组成年内科重症监护病房患者:对照组(2016 年至 2019 年入院;大流行前患者)、大流行 COVID-19 组 (PandeCOV) 和大流行非 COVID-19 组 (PandeCOV) 于 2020 年入院。主要结局是评估这些患者中与 VAP 相关的归因死亡率和归因分数。 使用具有因果推理的多状态建模,还评估了与 VAP 相关的结果。 共有 64816 名患者纳入对照组,7442 名患者纳入 PandeCOV 组,1687 名患者纳入 PandeCOV 组。每组每 1000 个通气日的 VAP 发生率分别为 14.2(95%置信区间 [CI],13.9 至 14.6)、18.3(95% CI,17.3 至 19.4)和 31.9(95% CI,29.8 至 34.2)。90 天的归因死亡率分别为 3.15%(95%CI,2.04%至 3.43%)、2.91%(95%CI,-0.21%至 5.02%)和 8.13%(95%CI,3.54%至 12.24%),90 天的归因死亡率分别为 1.22%(95%CI,0.83%至 1.63%)、1.42%(95%CI,-0.11%至 2.61%)和 9.17%(95%CI,3.54%至 12.24%)。除了发生 VAP 的风险较高外,PandeCOV 组与对照组具有相似的 VAP 特征。与对照组相比,PandeCOV 组无 VAP 患者的死亡风险较低(风险比,0.62;95%CI,0.52 至 0.74)。 COVID-19 患者的 VAP 归因死亡率较高,与 VAP 相关的总死亡率超过 9%。