Department of General & Neonatal Surgery, Children's Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders; Chongqing Key Laboratory of Pediatrics, Chongqing, China.
BMC Pediatr. 2022 May 10;22(1):259. doi: 10.1186/s12887-022-03333-y.
It has been shown that abnormalities of coagulation and fibrinolysis system are involved in the pathogenesis of necrotizing enterocolitis (NEC), but not well studied challenge in the context of early detection of disease progression. The present study mainly explores the predictive significance of coagulation parameters at the time of NEC diagnosis in identifying the patients who eventually received surgery and/or NEC-related deaths.
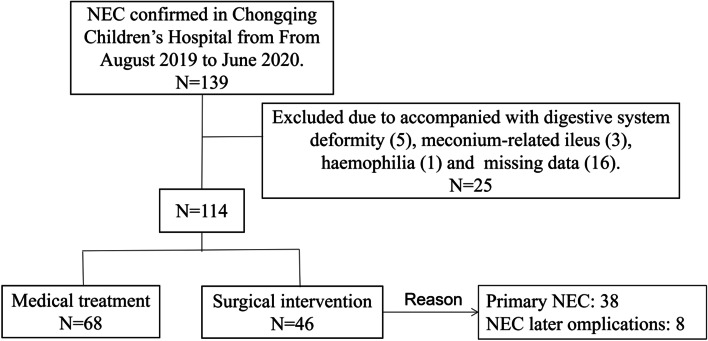
The retrospective study of 114 neonates with NEC was conducted with assessments of demographic data, laboratory results at the time of NEC diagnosis, treatment methods and prognosis. According to treatment methods, patients were divided into surgical intervention group and medical treatment group. Predictive factors were put forward and determined by receiver operating characteristic (ROC) curve analysis. An analysis of the surgical intervention and prognosis was performed.
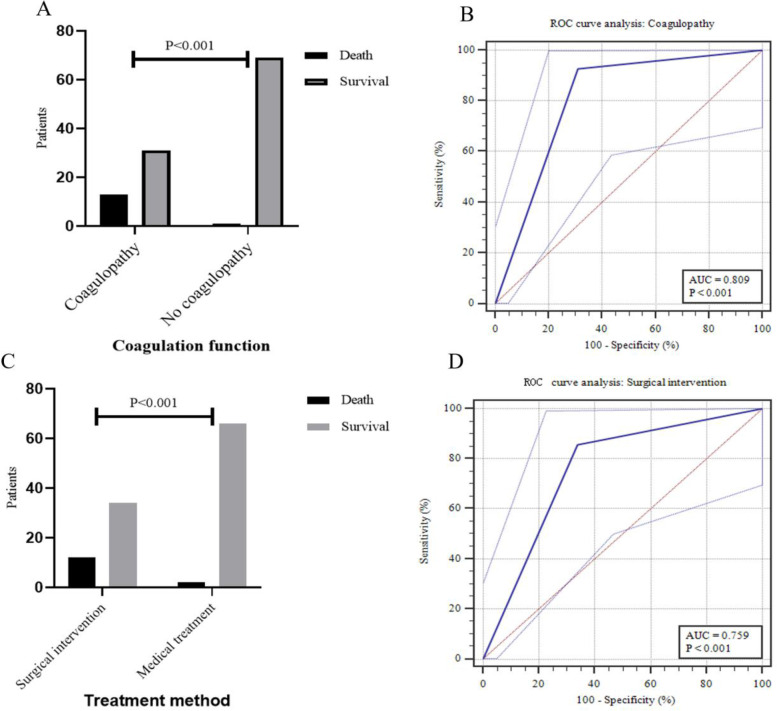
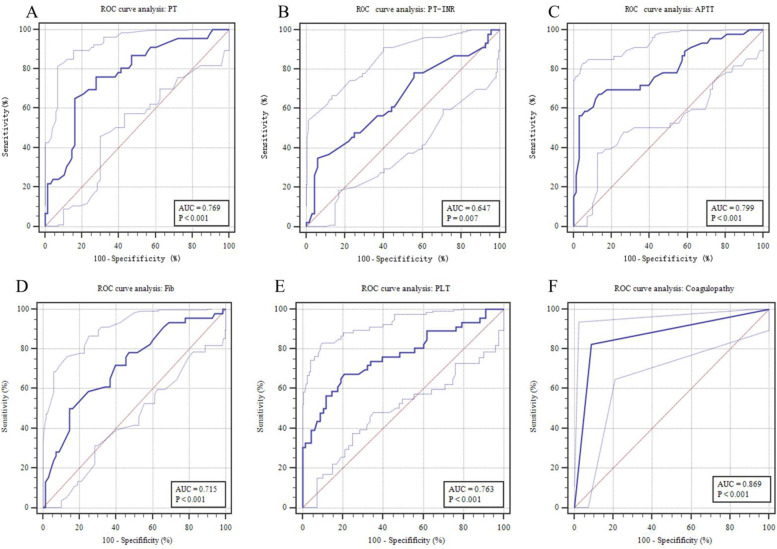
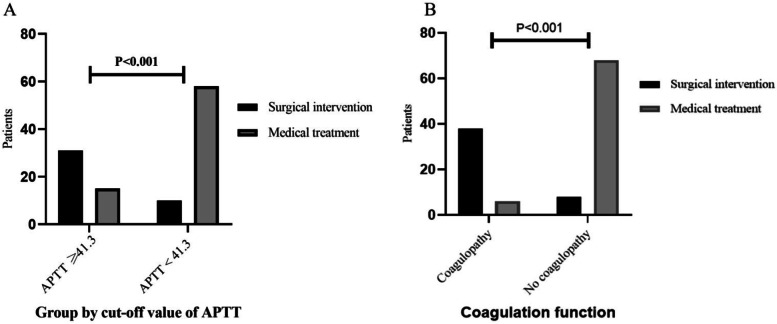
Of 114 patients, 46 (40.4%) cases received surgical intervention and 14 (12.3%) deaths. prothrombin time (PT), PT international normalized ratio, activated partial thromboplastin time (APTT), fibrinogen and platelet count at the time of NEC diagnosis were independently associated with surgical NEC. The APTT could identify patients at high risk for surgical NEC, with 67.39% sensitivity, 86.76% specificity, better than that of other serological parameters. Coagulopathy was found in 38.6% of all patients. For surgical intervention, the area under the ROC curve (AUC) of coagulopathy was 0.869 (95% confidence interval [CI]: 0.794 ~ 0.944, P < 0.001), with 82.61% sensitivity and 91.18% specificity, outperformed APTT (95% CI: 0.236 ~ 0.173, P = 0.001). Furthermore, the AUC for coagulopathy to predict mortality was 0.809 (95% CI: 0.725 ~ 0.877, P < 0.001), with 92.86% sensitivity and 69.0% specificity.
Coagulation parameters at the time of NEC diagnosis were conducive to early prediction of surgical NEC and -related deaths, which should be closely monitored in neonates at high risk of NEC and validated as a clinical decision-making tool.
已有研究表明,凝血和纤溶系统的异常参与了坏死性小肠结肠炎(NEC)的发病机制,但在疾病进展的早期检测方面研究甚少。本研究主要探讨 NEC 诊断时凝血参数的预测意义,以识别最终接受手术和/或与 NEC 相关死亡的患者。
对 114 例 NEC 新生儿进行回顾性研究,评估人口统计学数据、NEC 诊断时的实验室结果、治疗方法和预后。根据治疗方法,患者分为手术干预组和药物治疗组。通过受试者工作特征(ROC)曲线分析提出并确定预测因素。对手术干预和预后进行分析。
114 例患者中,46 例(40.4%)接受手术干预,14 例(12.3%)死亡。NEC 诊断时的凝血酶原时间(PT)、PT 国际标准化比值、活化部分凝血活酶时间(APTT)、纤维蛋白原和血小板计数与手术 NEC 独立相关。APTT 可识别手术 NEC 高危患者,其灵敏度为 67.39%,特异性为 86.76%,优于其他血清学参数。所有患者中有 38.6%存在凝血障碍。对于手术干预,凝血障碍的 ROC 曲线下面积(AUC)为 0.869(95%置信区间 [CI]:0.7940.944,P<0.001),灵敏度为 82.61%,特异性为 91.18%,优于 APTT(95%CI:0.2360.173,P=0.001)。此外,凝血障碍预测死亡率的 AUC 为 0.809(95%CI:0.725~0.877,P<0.001),灵敏度为 92.86%,特异性为 69.0%。
NEC 诊断时的凝血参数有助于早期预测手术 NEC 及相关死亡,对于 NEC 高危新生儿应密切监测,并验证其作为临床决策工具的价值。