Alhariri Sara, Kalas M Ammar, Hassan Mariam, Carter Jordan T, Ghafouri S Reshad, Dihowm Fatma
Internal Medicine, Texas Tech University Health Sciences Center El Paso, El Paso, USA.
Orthopaedics, University of Texas Health Science Center at San Antonio, San Antonio, USA.
Cureus. 2022 Apr 9;14(4):e23969. doi: 10.7759/cureus.23969. eCollection 2022 Apr.
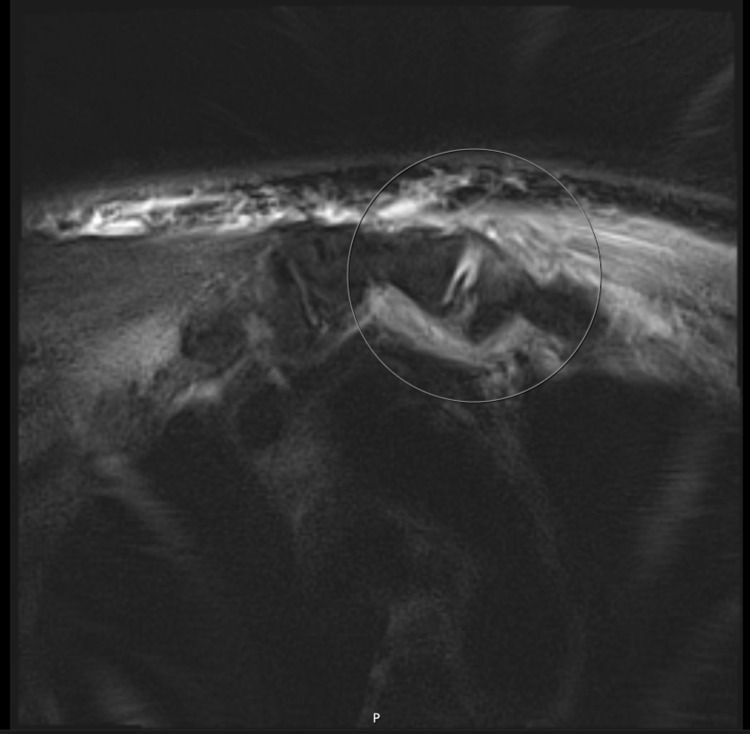
The sternoclavicular joint (SCJ) is an uncommon location for septic arthritis to occur in. Due to the rarity of the condition and the nonspecific symptoms, SCJ septic arthritis can be missed or mislabeled as osteoarthritis or muscle strain. Accurate history and physical examination is crucial for recognizing this condition. With the potential life-threatening complications that may ensue, SCJ septic arthritis has traditionally been managed surgically. This ranges from simple incision and drainage to resection of the joint. However, in cases where there is not enough fluid for incision and drainage, a trial of medical management with antibiotics can be attempted. We herein describe a case of a 58-year-old male who presented with nonspecific anterior chest wall and neck pain. Chest X-ray and ultrasound of the anterior chest wall was normal; however, magnetic resonance imaging (MRI) of the chest showed a small effusion without other complications. His blood cultures grew extended-spectrum beta-lactamase (ESBL)-producing rendering this as his hematogenous source of septic arthritis. The ESBL was from a left-sided obstructing kidney stone that resulted in pyelonephritis, which was confirmed via computed tomography of the abdomen. His effusion was too minimal to drain; therefore, he was managed medically with intravenous (IV) antibiotics along with a left ureteral stent placement, and he had a full recovery. This case represents the ability for SCJ septic arthritis to be managed medically with IV antibiotics, especially when the diagnosis is caught early without complications. The role of MRI is indispensable for coming to the diagnosis, as it is capable of detecting complications that ultimately dictate management. Additionally, this case highlights the unique microorganism, ESBL-producing causing the SCJ septic arthritisa finding that has been rarely reported in the literature as the majority of microorganisms that have been previously documented are either or
胸锁关节(SCJ)是化脓性关节炎发生的罕见部位。由于这种疾病罕见且症状不具特异性,胸锁关节化脓性关节炎可能会被漏诊或误诊为骨关节炎或肌肉拉伤。准确的病史和体格检查对于识别这种疾病至关重要。鉴于可能随之而来的危及生命的并发症,传统上胸锁关节化脓性关节炎采用手术治疗。范围从简单的切开引流到关节切除。然而,在没有足够液体进行切开引流的情况下,可以尝试使用抗生素进行药物治疗试验。我们在此描述一例58岁男性患者,他表现为非特异性的前胸壁和颈部疼痛。前胸壁的胸部X线和超声检查正常;然而,胸部磁共振成像(MRI)显示有少量积液,无其他并发症。他的血培养结果显示产超广谱β-内酰胺酶(ESBL),这表明这是他化脓性关节炎的血源性病因。ESBL来自左侧阻塞性肾结石,导致肾盂肾炎,通过腹部计算机断层扫描得以证实。他的积液太少无法引流;因此,对他进行了静脉注射(IV)抗生素治疗并放置了左输尿管支架,他完全康复了。这个病例表明胸锁关节化脓性关节炎可以用静脉注射抗生素进行药物治疗,特别是在早期诊断且无并发症的情况下。MRI在诊断中起着不可或缺的作用,因为它能够检测到最终决定治疗方案的并发症。此外,这个病例突出了导致胸锁关节化脓性关节炎的独特微生物——产ESBL菌,这一发现很少在文献中报道,因为之前记录的大多数微生物要么是……要么是……