Walter-Nicolet Elizabeth, Marchand-Martin Laetitia, Guellec Isabelle, Biran Valérie, Moktari Mostafa, Zana-Taieb Elodie, Magny Jean-François, Desfrère Luc, Waszak Paul, Boileau Pascal, Chauvin Gilles, de Saint Blanquat Laure, Borrhomée Suzanne, Droutman Stéphanie, Merhi Mona, Zupan Véronique, Karoui Leila, Cimerman Patricia, Carbajal Ricardo, Durrmeyer Xavier
Medicine and Neonatal Intensive Care Unit Saint Joseph Hospital Paris France.
INSERM U1153, Epidemiology and Statistics Sorbonne Paris Cité Research Center Obstetrical, Perinatal and Pediatric Epidemiology Team Paris France.
Paediatr Neonatal Pain. 2021 Apr 4;3(2):46-58. doi: 10.1002/pne2.12048. eCollection 2021 Jun.
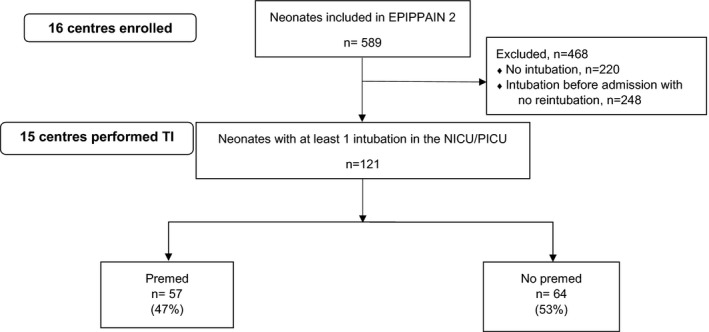
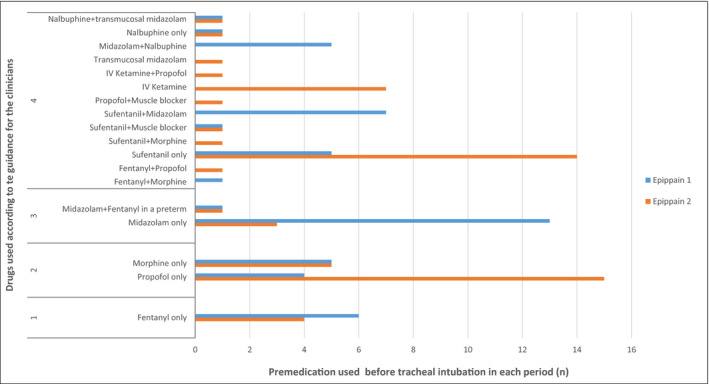
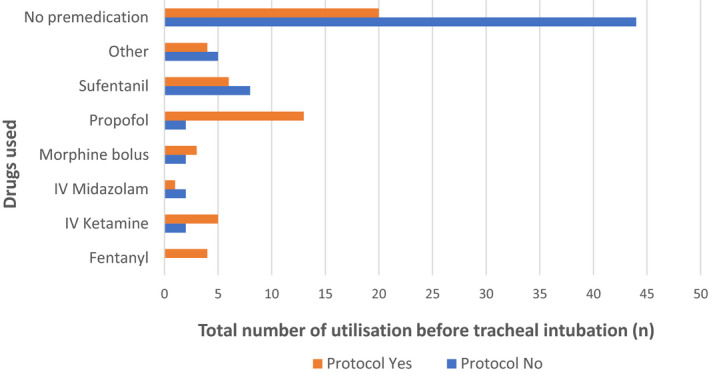
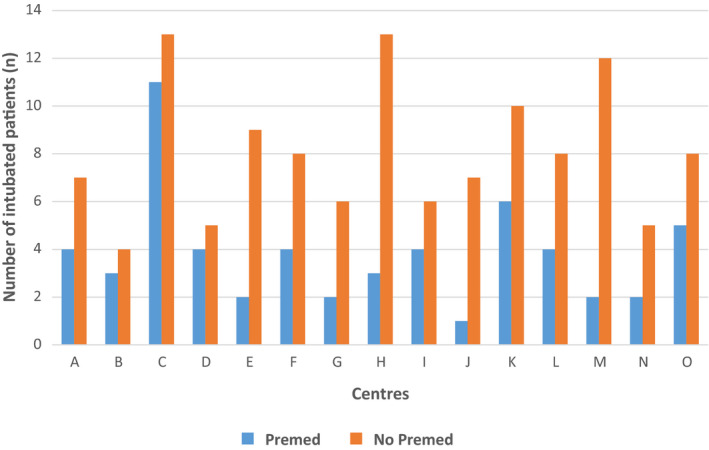
To describe the frequency and nature of premedication practices for neonatal tracheal intubation (TI) in 2011; to identify independent risk factors for the absence of premedication; to compare data with those from 2005 and to confront observed practices with current recommendations. Data concerning TI performed in neonates during the first 14 days of their admission to participating neonatal/pediatric intensive care units were prospectively collected at the bedside. This study was part of the Epidemiology of Procedural Pain in Neonates study (EPIPPAIN 2) conducted in 16 tertiary care units in the region of Paris, France, in 2011. Multivariate analysis was used to identify factors associated with premedication use and multilevel analysis to identify center effect. Results were compared with those of the EPIPPAIN 1 study, conducted in 2005 with a similar design, and to a current guidance for the clinician for this procedure. One hundred and twenty-one intubations carried out in 121 patients were analyzed. The specific premedication rate was 47% and drugs used included mainly propofol (26%), sufentanil (24%), and ketamine (12%). Three factors were associated with the use of a specific premedication: nonemergent TI (Odds ratio (OR) [95% CI]: 5.3 [1.49-20.80]), existence of a specific written protocol in the ward (OR [95% CI]:4.80 [2.12-11.57]), and the absence of a nonspecific concurrent analgesia infusion before TI (OR [95% CI]: 3.41 [1.46-8.45]). No center effect was observed. The specific premedication rate was lower than the 56% rate observed in 2005. The drugs used were more homogenous and consistent with the current recommendations than in 2005, especially in centers with a specific written protocol. Premedication use prior to neonatal TI was low, even for nonemergent procedures. Scientific consensus, implementation of international or national recommendations, and local written protocols are urgently needed to improve premedication practices for neonatal intubation.
描述2011年新生儿气管插管(TI)术前用药的频率和性质;确定未进行术前用药的独立危险因素;将数据与2005年的数据进行比较,并将观察到的做法与当前建议进行对照。在参与研究的新生儿/儿科重症监护病房,对新生儿入院后头14天内进行的TI相关数据在床边进行前瞻性收集。本研究是2011年在法国巴黎地区16个三级医疗机构开展的新生儿程序性疼痛流行病学研究(EPIPPAIN 2)的一部分。采用多变量分析确定与术前用药相关的因素,采用多水平分析确定中心效应。将结果与2005年采用类似设计开展的EPIPPAIN 1研究的结果以及该操作当前的临床医生指南进行比较。对121例患者进行的121次气管插管进行了分析。特异性术前用药率为47%,使用的药物主要包括丙泊酚(26%)、舒芬太尼(24%)和氯胺酮(12%)。三个因素与特异性术前用药的使用相关:非紧急TI(比值比(OR)[95%可信区间]:5.3[1.49 - 20.80])、病房存在特异性书面方案(OR[95%可信区间]:4.80[2.12 - 11.57])以及TI前未进行非特异性同时镇痛输注(OR[95%可信区间]:3.41[1.46 - 8.45])。未观察到中心效应。特异性术前用药率低于2005年观察到的56%的比率。与2005年相比,使用的药物更具同质性且符合当前建议,尤其是在有特异性书面方案的中心。新生儿TI前的术前用药使用率较低,即使对于非紧急手术也是如此。迫切需要科学共识、国际或国家建议的实施以及地方书面方案来改善新生儿插管的术前用药做法。