Department of Gastroenterology, Princess Alexandra and Mater Hospitals, and Faculty of Medicine, The University of Queensland, Brisbane, QLD, Australia.
QIMR Berghofer Medical Research Institute, and Faculty of Medicine, The University of Queensland, Brisbane, QLD, Australia.
Dig Dis Sci. 2023 Jan;68(1):291-303. doi: 10.1007/s10620-022-07483-y. Epub 2022 May 13.
In 2016, direct-acting antiviral (DAA) treatment for hepatitis C (HCV) became available through Australia's universal health care system, with the aim of HCV elimination. We report real-world effectiveness of DAA HCV treatment in Australia from a clinically well-informed cohort, enriched for cirrhosis and prior HCV treatment.
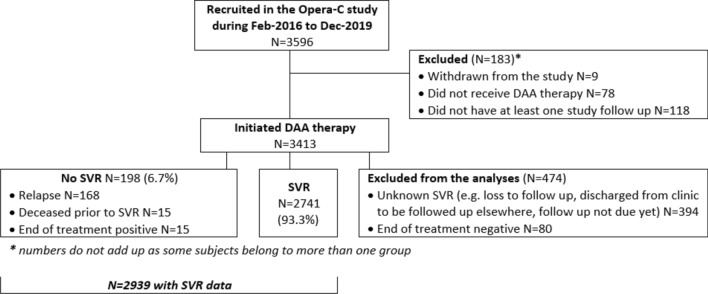
3413 patients were recruited from 26 hospital liver clinics across Australia from February 2016 to June 2020. Clinical history and sustained viral response (SVR) were obtained from medical records and data linkage to the Australian Pharmaceutical Benefits Scheme. Factors associated with SVR were assessed by multivariable logistic regression (MVR).
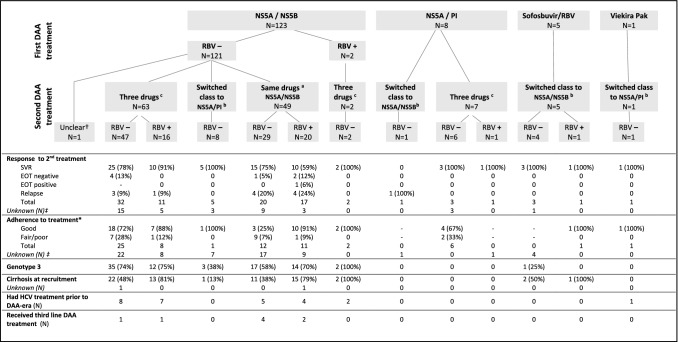
At recruitment, 32.2% had cirrhosis (72.9% Child Pugh class B/C), and 19.9% were treatment experienced. Of the 2,939 with data, 93.3% confirmed SVR. 137 patients received second-line therapy. Patients with cirrhosis had lower SVR rate (88.4 vs. 95.8%; p < 0.001). On MVR, failure to achieve SVR was associated with Genotype 3 (adj-OR = 0.42, 95%CI 0.29-0.61), male gender (adj-OR = 0.49, 95%CI 0.31-0.77), fair/poor adherence (adj-OR = 0.52, 95%CI 0.28-0.94), cirrhosis (adj-OR = 0.57, 95%CI 0.36-0.88), FIB-4 > 3.25 (adj-OR = 0.52, 95%CI 0.33-0.83) and MELD score ≥ 20 (adj-OR = 0.25, 95%CI 0.08-0.80). Consistent results were seen in cirrhotic sub-analysis.
Excellent SVR rates were achieved with DAAs in this real-world cohort of patients with chronic HCV infection. More advanced liver disease and clinician impression of poor adherence were associated with HCV treatment failure. Supports to improve liver fibrosis assessment skills for non-specialist DAA prescribers in the community and to optimize patient adherence are likely to enable more effective pursuit of HCV elimination in Australia.
2016 年,澳大利亚全民医保体系开始提供直接作用抗病毒药物(DAA)治疗丙型肝炎(HCV),旨在消除 HCV。我们报告了在临床知情队列中从澳大利亚 DAA HCV 治疗的真实有效性,该队列富集了肝硬化和既往 HCV 治疗患者。
2016 年 2 月至 2020 年 6 月期间,从澳大利亚 26 家医院肝脏诊所招募了 3413 名患者。临床病史和持续病毒应答(SVR)从病历中获得,并通过数据链接到澳大利亚药品福利计划。采用多变量逻辑回归(MVR)评估 SVR 的相关因素。
在招募时,32.2%的患者有肝硬化(72.9%的患者为 Child Pugh 级 B/C),19.9%的患者有既往治疗史。在有数据的 2939 名患者中,93.3%的患者确认 SVR。137 名患者接受二线治疗。肝硬化患者 SVR 率较低(88.4%与 95.8%;p<0.001)。MVR 分析表明,未能实现 SVR 与基因型 3(调整比值比[OR]=0.42,95%CI 0.29-0.61)、男性(调整 OR=0.49,95%CI 0.31-0.77)、中等/差的依从性(调整 OR=0.52,95%CI 0.28-0.94)、肝硬化(调整 OR=0.57,95%CI 0.36-0.88)、FIB-4>3.25(调整 OR=0.52,95%CI 0.33-0.83)和 MELD 评分≥20(调整 OR=0.25,95%CI 0.08-0.80)有关。在肝硬化亚组分析中也得到了一致的结果。
在澳大利亚,真实世界队列中,慢性 HCV 感染患者使用 DAA 治疗获得了优异的 SVR 率。更严重的肝脏疾病和临床医生对依从性差的印象与 HCV 治疗失败有关。支持提高社区非专科 DAA 开处方者对肝纤维化评估技能,并优化患者依从性,可能会使澳大利亚更有效地实现 HCV 消除。