Melchers Max, van Zanten Arthur R H, Heusinkveld Moniek, Leeuwis Jan Willem, Schellaars Roel, Lammers Hendrick J W, Kreemer Freek J, Haas Pieter-Jan, Verweij Paul E, van Bree Sjoerd H W
Department of Intensive Care Medicine, Gelderse Vallei Hospital, Ede, The Netherlands.
Division of Human Nutrition and Health, Wageningen University & Research, Wageningen, The Netherlands.
Crit Care Explor. 2022 May 9;4(5):e0696. doi: 10.1097/CCE.0000000000000696. eCollection 2022 May.
Despite high mortality rates of COVID-19-associated pulmonary aspergillosis (CAPA) in the ICU, antifungal prophylaxis remains a subject of debate. We initiated nebulized conventional amphotericin B (c-AmB) as antifungal prophylaxis in COVID-19 patients on invasive mechanical ventilation (IMV).
To assess the CAPA incidence in COVID-19 patients on IMV treated with and without nebulized c-AmB as antifungal prophylaxis.
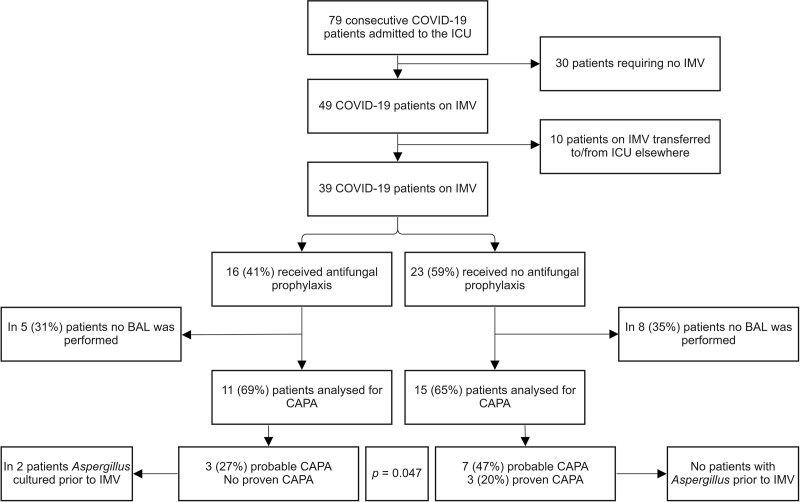
Retrospective cohort study of consecutive COVID-19 patients admitted to our adult 17-bed ICU in a university-affiliated general hospital in Ede, The Netherlands, between January 25, 2021, and July 9, 2021. Patients not requiring IMV or transferred from or to another ICU were excluded. From April 9, 2021, daily nebulized amphotericin B in all patients on IMV was initiated.
Bronchoscopy with bronchoalveolar lavage (BAL) was performed in case of positive cultures for from the respiratory tract and/or unexplained respiratory deterioration. Incidence of probable and proven CAPA was compared between patients treated with and without nebulized antifungal prophylaxis using Pearson chi-square test.
A total of 39 intubated COVID-19 patients could be analyzed, of which 16 were treated with antifungal prophylaxis and 23 were not. Twenty-six patients underwent bronchoscopy with BAL. In patients treated with antifungal prophylaxis, the incidence of probable/proven CAPA was significantly lower when compared with no antifungal prophylaxis (27% vs 67%; = 0.047). Incidence of tracheobronchial lesions and positive cultures and BAL-galactomannan was significantly lower in patients treated with antifungal prophylaxis (9% vs 47%; = 0.040, 9% vs 53%; = 0.044, and 20% vs 60%; = 0.047, respectively). No treatment-related adverse events and no case of proven CAPA were encountered in patients receiving antifungal prophylaxis.
Nebulization of c-AmB in critically ill COVID-19 patients on IMV is safe and may be considered as antifungal prophylaxis to prevent CAPA. However, a randomized controlled trial to confirm this is warranted.
尽管重症监护病房(ICU)中与新冠病毒相关的肺曲霉病(CAPA)死亡率很高,但抗真菌预防措施仍是一个有争议的话题。我们对接受有创机械通气(IMV)的新冠患者启动了雾化常规两性霉素B(c-AmB)作为抗真菌预防措施。
评估接受和未接受雾化c-AmB抗真菌预防治疗的IMV新冠患者中CAPA的发病率。
设计、地点和参与者:对2021年1月25日至2021年7月9日期间入住荷兰埃德市一家大学附属医院拥有17张床位的成人ICU的连续新冠患者进行回顾性队列研究。排除不需要IMV或从其他ICU转入或转出的患者。从2021年4月9日起,对所有接受IMV的患者开始每日雾化两性霉素B治疗。
如果呼吸道培养阳性和/或出现无法解释的呼吸功能恶化,则进行支气管镜检查及支气管肺泡灌洗(BAL)。使用Pearson卡方检验比较接受和未接受雾化抗真菌预防治疗的患者中可能和确诊的CAPA发病率。
总共可以分析39例插管新冠患者,其中16例接受了抗真菌预防治疗,23例未接受。26例患者接受了支气管镜检查及BAL。接受抗真菌预防治疗的患者中,可能/确诊的CAPA发病率与未接受抗真菌预防治疗的患者相比显著更低(27%对67%;P = 0.047)。接受抗真菌预防治疗的患者气管支气管病变、培养阳性及BAL半乳甘露聚糖阳性的发病率显著更低(分别为9%对47%;P = 0.04)、(9%对53%;P = 0.044)、(20%对60%;P = 0.047)。接受抗真菌预防治疗的患者未出现与治疗相关的不良事件,也未出现确诊的CAPA病例。
对接受IMV的重症新冠患者雾化c-AmB是安全的,可考虑作为预防CAPA的抗真菌预防措施。然而,需要进行一项随机对照试验来证实这一点。