Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, UW Health Hospital and Clinics, and the Department of Statistics and the Department of Biostatistics & Medical Informatics, University of Wisconsin-Madison, Madison, Wisconsin.
Obstet Gynecol. 2022 May 1;139(5):735-744. doi: 10.1097/AOG.0000000000004732. Epub 2022 Apr 5.
To perform an updated Markov modeling to assess the optimal age for bilateral salpingo-oophorectomy (BSO) at the time of hysterectomy for benign indication.
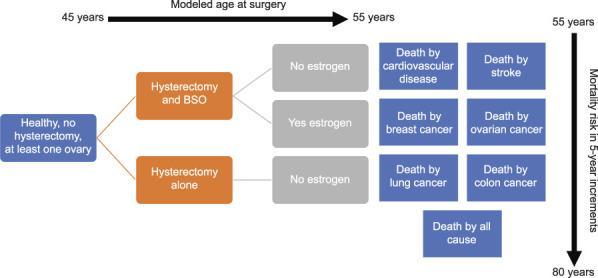
We performed a literature review that assessed hazard ratios (HRs) for mortality by disease, age, hysterectomy with or without BSO, and estrogen therapy use. Base mortality rates were derived from national vital statistics data. A Markov model from reported HRs predicted the proportion of the population staying alive to age 80 years by 1-year and 5-year age groups at time of surgery, from age 45 to 55 years. Those younger than age 50 years were modeled as either taking postoperative estrogen or not; those 50 and older were modeled as not receiving estrogen. Computations were performed with R 3.5.1, using Bayesian integration for HR uncertainty.
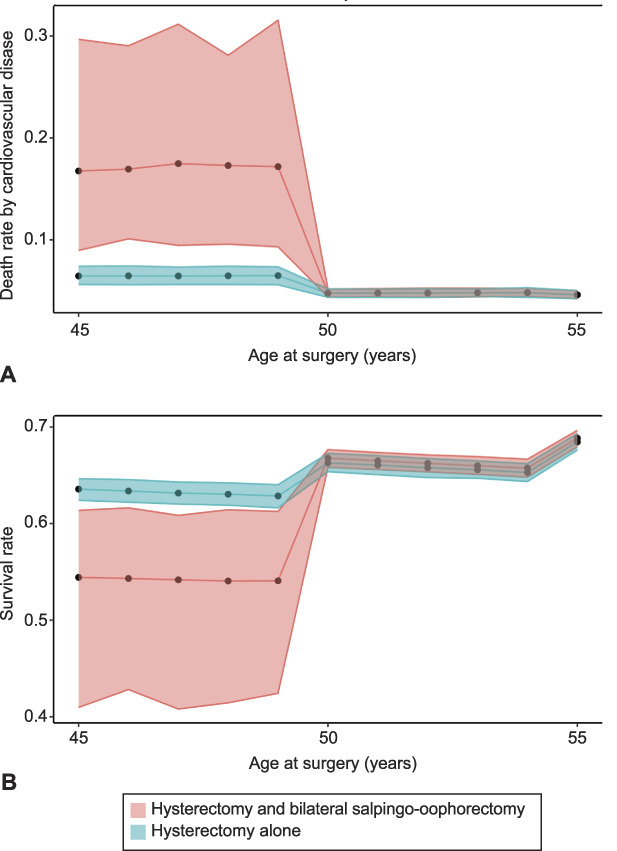
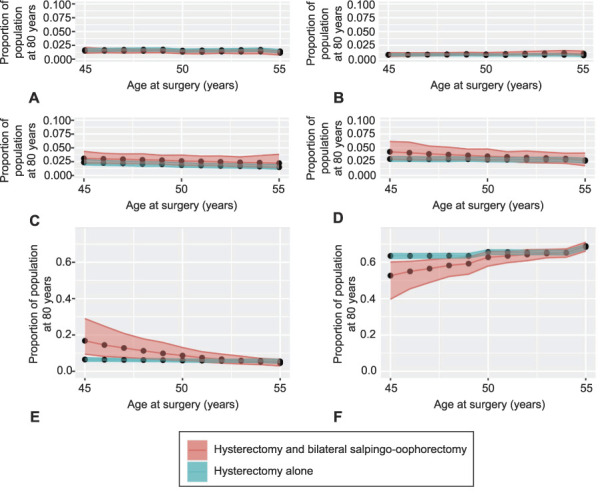
Performing salpingo-oophorectomy before age 50 years for those not taking estrogen yields a lower survival proportion to age 80 years than hysterectomy alone before age 50 years (52.8% [Bayesian CI 40.7-59.7] vs 63.5% [Bayesian CI 62.2-64.9]). At or after age 50 years, there were similar proportions of those living to age 80 years with hysterectomy alone (66.4%, Bayesian CI 65.0-67.6) compared with concurrent salpingo-oophorectomy (66.9%, Bayesian CI 64.4-69.0). Importantly, those taking estrogen when salpingo-oophorectomy was performed before age 50 years had similar proportions of cardiovascular disease, stroke, and people living to age 80 years as those undergoing hysterectomy alone or those undergoing hysterectomy and salpingo-oophorectomy at age 50 years and older.
This updated Markov model argues for the consideration of concurrent salpingo-oophorectomy for patients who are undergoing hysterectomy at age 50 and older and suggests that initiating estrogen in those who need salpingo-oophorectomy before age 50 years mitigates increased mortality risk.
通过更新马尔可夫模型来评估因良性指征行子宫切除术时行双侧输卵管卵巢切除术(BSO)的最佳年龄。
我们进行了文献回顾,评估了疾病、年龄、行或不行 BSO 的子宫切除术以及雌激素治疗使用与死亡率的危险比(HR)。基础死亡率来源于国家生命统计数据。根据报道的 HR,马尔可夫模型预测了从 45 岁到 55 岁手术时,1 岁和 5 岁年龄组人群到 80 岁的存活比例。50 岁以下的人群被建模为是否接受术后雌激素治疗;50 岁及以上的人群被建模为不接受雌激素治疗。使用 R 3.5.1 进行计算,使用贝叶斯积分来处理 HR 不确定性。
对于不接受雌激素治疗的人群,在 50 岁之前行 BSO 手术比在 50 岁之前单独行子宫切除术的生存比例更低(52.8%[贝叶斯 CI 40.7-59.7] vs 63.5%[贝叶斯 CI 62.2-64.9])。在 50 岁及以上,单独行子宫切除术(66.4%,贝叶斯 CI 65.0-67.6)与同期行 BSO 手术(66.9%,贝叶斯 CI 64.4-69.0)的人群到 80 岁的存活比例相似。重要的是,在 50 岁之前行 BSO 手术并接受雌激素治疗的人群,其心血管疾病、中风发病率以及到 80 岁的存活比例与单独行子宫切除术或 50 岁及以上同期行子宫切除术和 BSO 手术的人群相似。
该更新的马尔可夫模型支持对 50 岁及以上行子宫切除术的患者考虑同期行 BSO 手术,并建议在 50 岁之前需要行 BSO 的患者开始接受雌激素治疗,以减轻死亡率增加的风险。