Department of Anesthesiology, Nanjing Second Hospital, Nanjing, Jiangsu, China.
Nanjing Hospital Affiliated to Nanjing University of Chinese Medicine, Nanjing University of Chinese Medicine, Nanjing, Jangsu, China.
BMJ Open. 2022 May 18;12(5):e051112. doi: 10.1136/bmjopen-2021-051112.
To evaluate the reliability of stroke volume variation (SVV) for predicting responsiveness to fluid therapy in patients undergoing cardiac and thoracic surgery.
Systematic review and meta-analysis.
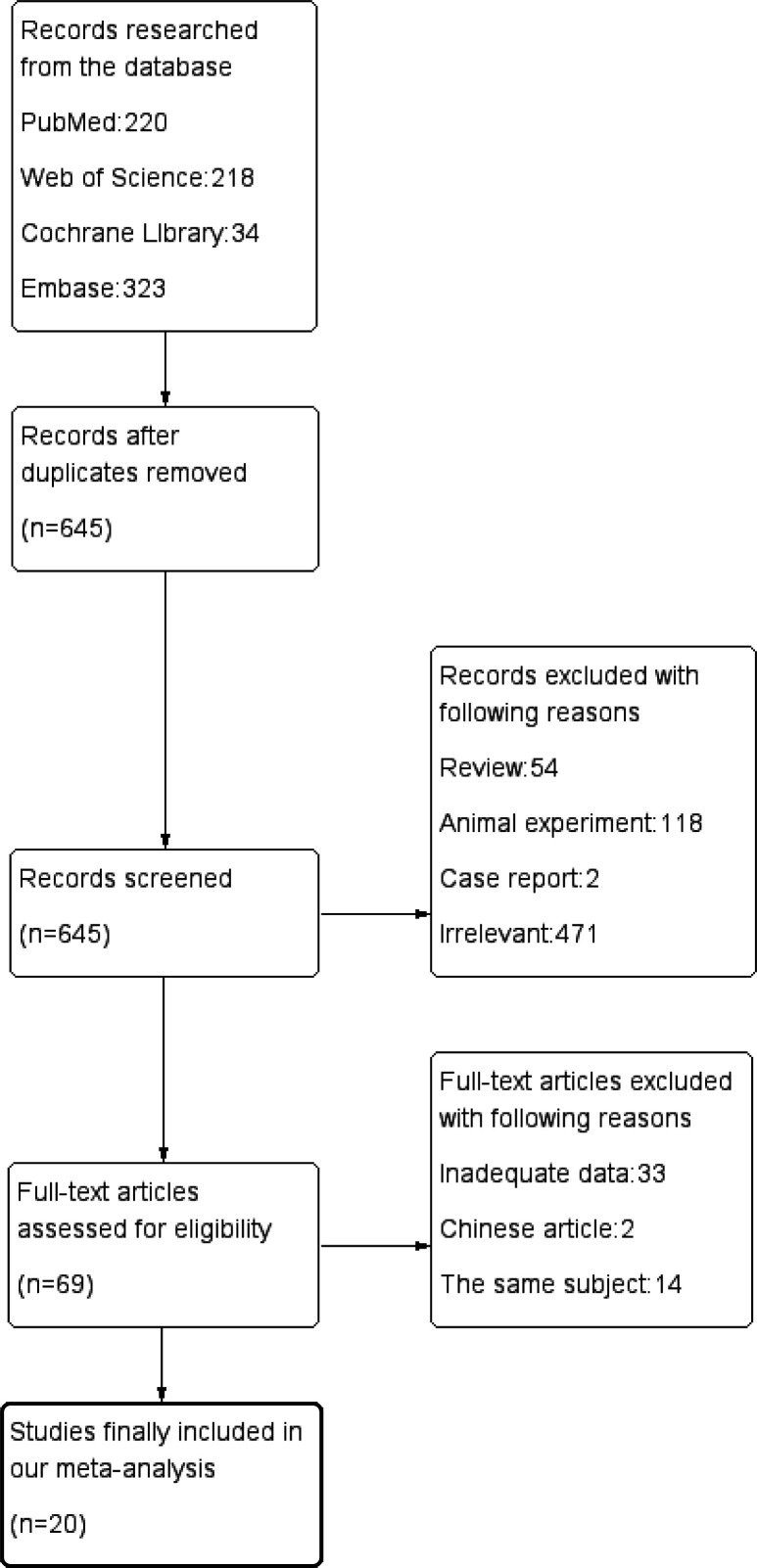
PubMed, EMBASE, Cochrane Library, Web of Science up to 9 August 2020.
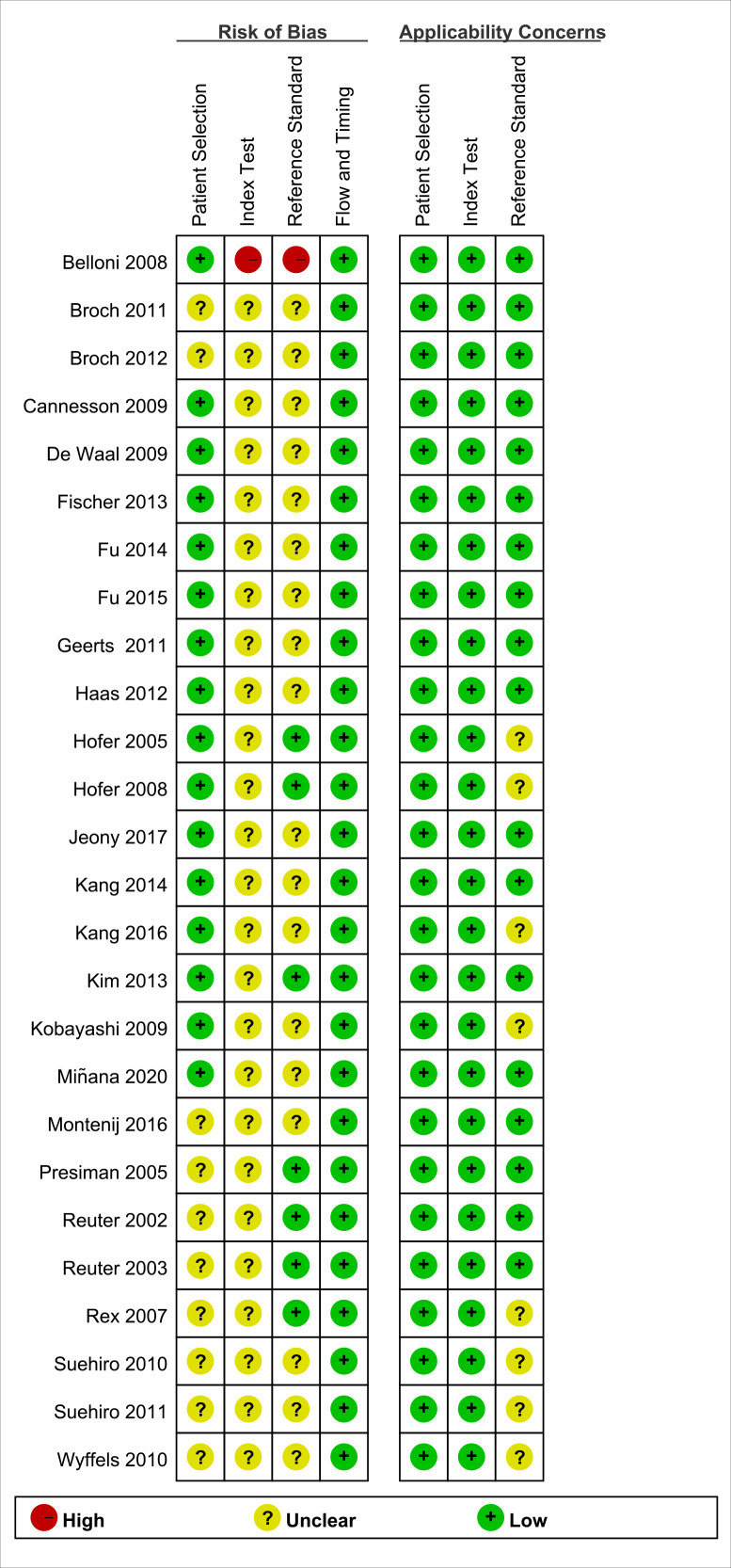
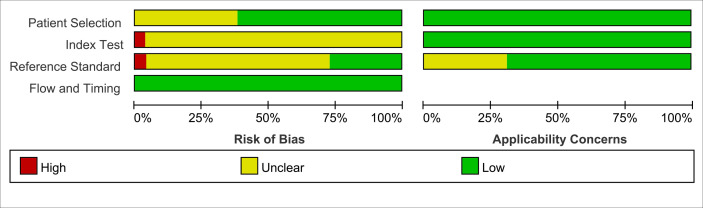
Quality of included studies were assessed with the Quality Assessment of Diagnostic Accuracy Studies-2 tool. We conducted subgroup analysis according to different anaesthesia and surgical methods with Stata V.14.0, Review Manager V.5.3 and R V.3.6.3. We used random-effects model to pool sensitivity, specificity and diagnostic odds ratio with 95% CI. The area under the curve (AUC) of receiver operating characteristic was calculated.
Among the 20 relevant studies, 7 were conducted during thoracic surgery, 8 were conducted during cardiac surgery and the remaining 5 were conducted in intensive critical unit (ICU) after cardiac surgery. Data from 854 patients accepting mechanical ventilation were included in our systematic review. The pooled sensitivity and specificity were 0.73 (95% CI: 0.59 to 0.83) and 0.62 (95% CI: 0.46 to 0.76) in the thoracic surgery group, 0.71 (95% CI: 0.65 to 0.77) and 0.76 (95% CI: 0.69 to 0.82) in the cardiac surgery group, 0.85 (95% CI: 0.60 to 0.96) and 0.85 (95% CI: 0.74 to 0.92) in cardiac ICU group. The AUC was 0.73 (95% CI: 0.69 to 0.77), 0.80 (95% CI: 0.77 to 0.83) and 0.88 (95% CI: 0.86 to 0.92), respectively. Results of subgroup of FloTrac/Vigileo system (AUC=0.80, Youden index=0.38) and large tidal volume (AUC=0.81, Youden index=0.48) in thoracic surgery, colloid (AUC=0.85, Youden index=0.55) and postoperation (AUC=0.85, Youden index=0.63) in cardiac surgery, passive leg raising (AUC=0.90, Youden index=0.72) in cardiac ICU were reliable.
SVV had good predictive performance in cardiac surgery or ICU after cardiac surgery and had moderate predictive performance in thoracic surgery. Nevertheless, technical and clinical variables may affect the predictive value potentially.
评估每搏量变异度(SVV)预测心脏和胸外科手术患者对液体治疗反应的可靠性。
系统评价和荟萃分析。
PubMed、EMBASE、Cochrane 图书馆、Web of Science 截至 2020 年 8 月 9 日。
使用诊断准确性研究质量评估工具 2 对纳入研究的质量进行评估。我们使用 Stata V.14.0、Review Manager V.5.3 和 R V.3.6.3 根据不同的麻醉和手术方法进行亚组分析。使用随机效应模型以 95%置信区间(CI)汇总敏感度、特异度和诊断比值比。计算接收者操作特征曲线下面积(AUC)。
在 20 项相关研究中,有 7 项在胸外科手术期间进行,8 项在心脏手术期间进行,其余 5 项在心脏手术后的重症监护病房(ICU)进行。我们的系统评价纳入了 854 例接受机械通气的患者的数据。在胸外科手术组中,SVV 的汇总敏感度和特异度分别为 0.73(95%CI:0.59 至 0.83)和 0.62(95%CI:0.46 至 0.76),在心脏手术组中,SVV 的汇总敏感度和特异度分别为 0.71(95%CI:0.65 至 0.77)和 0.76(95%CI:0.69 至 0.82),在心脏 ICU 组中,SVV 的汇总敏感度和特异度分别为 0.85(95%CI:0.60 至 0.96)和 0.85(95%CI:0.74 至 0.92)。AUC 分别为 0.73(95%CI:0.69 至 0.77)、0.80(95%CI:0.77 至 0.83)和 0.88(95%CI:0.86 至 0.92)。胸外科手术中 FloTrac/Vigileo 系统(AUC=0.80,Youden 指数=0.38)和大潮气量(AUC=0.81,Youden 指数=0.48)、心脏手术中胶体(AUC=0.85,Youden 指数=0.55)和术后(AUC=0.85,Youden 指数=0.63)以及心脏 ICU 中的被动抬腿(AUC=0.90,Youden 指数=0.72)的亚组分析结果可靠。
SVV 在心脏手术或心脏手术后的 ICU 中具有良好的预测性能,在胸外科手术中具有中等的预测性能。然而,技术和临床变量可能会对预测值产生潜在影响。