International Institute for Population Sciences, Mumbai, India.
Department of Population and Development, International Institute for Population Sciences, Mumbai, India.
BMC Health Serv Res. 2022 May 18;22(1):670. doi: 10.1186/s12913-022-07984-6.
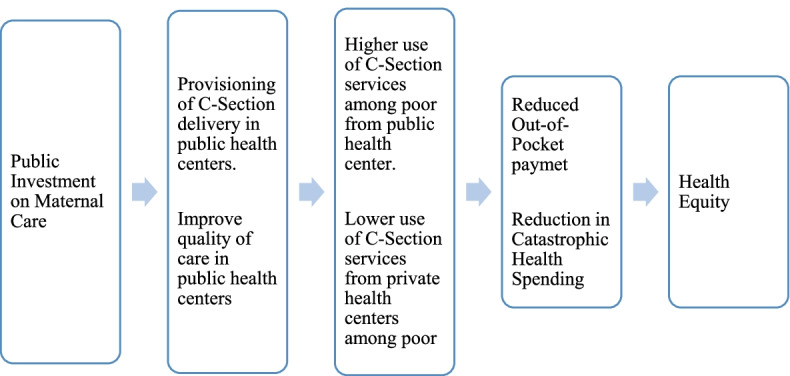
In the last two decades, cesarean section (CS) deliveries in India have increased by six-fold and created economic hardship for families and households. Although several schemes and policies under the National Health Mission (NHM) have reduced the inequality in the use of maternal care services in India, the distributive effect of public health subsidies on CS deliveries remains unclear. In this context, this paper examines the usage patterns of CS delivery and estimates the share of public health subsidies on CS deliveries among mothers by different background characteristics in India.
Data from the fourth round of the National Family Health Survey (NFHS-4) was used for the study. Out-of-pocket (OOP) payment for CS delivery was used as a dependent variable and was analyzed by level of care that is, primary (PHC, UHC, other) and secondary (government/municipal, rural hospital). Descriptive statistics, binary logistic regression, benefit incidence analysis, concentration curve and concentration index were used for the analysis.
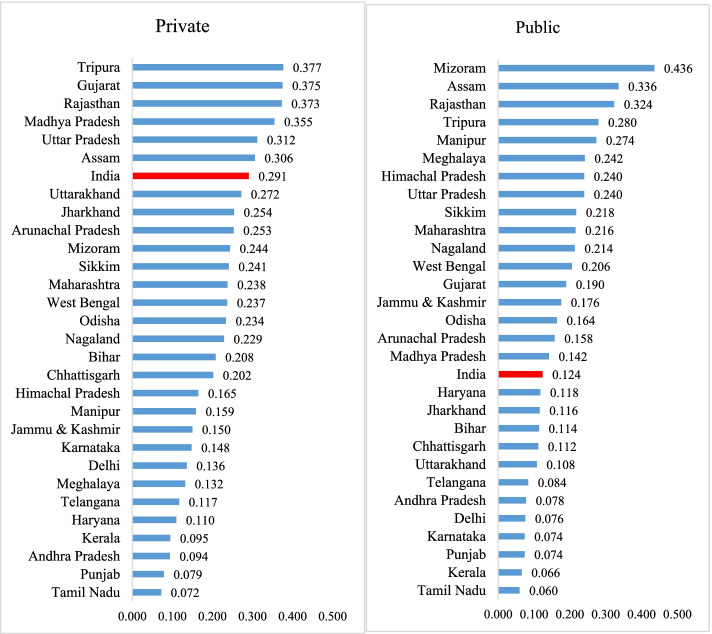
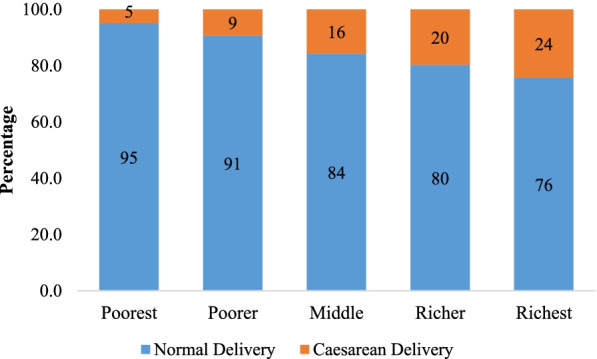
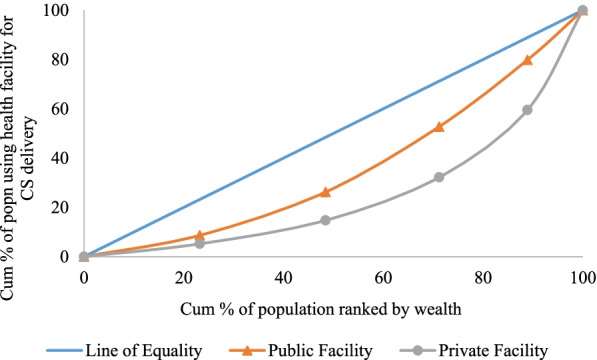
A strong economic gradient was observed in the utilization of CS delivery from public health facilities. Among mothers using any public health facility, 23% from the richest quintile did not pay for CS delivery compared to 13% from the poorest quintile. The use of the public subsidy among mothers using any type of public health facility for CS delivery was pro-rich in nature; 9% in the poorest quintile, 16.1% in the poorer, 24.5% in the middle, 27.5% among richer and 23% in the richest quintile. The pattern of utilization and distribution of public subsidy was similar across the primary and secondary health facilities but the magnitude varied. The findings from the benefit-incidence analysis are supported by those obtained from the inequality analysis. The concentration index of CS was 0.124 for public health centers and 0.291 for private health centers. The extent of inequality in the use of CS delivery in public health centers was highest in the state of Mizoram (0.436), followed by Assam (0.336), and the lowest in Tamil Nadu (0.060), followed by Kerala (0.066).
The utilization of CS services from public health centers in India is pro-rich. Periodically monitoring and evaluating of the cash incentive schemes for CS delivery and generating awareness among the poor would increase the use of CS delivery services in public health centers and reduce the inequality in CS delivery in India.
在过去的二十年中,印度的剖宫产(CS)分娩增加了六倍,给家庭和家庭带来了经济困难。尽管国家健康使命(NHM)下的几项计划和政策减少了印度产妇护理服务使用方面的不平等,但公共卫生补贴对 CS 分娩的分配效果仍不清楚。在这种情况下,本文研究了 CS 分娩的使用模式,并估计了按不同背景特征的印度母亲的 CS 分娩中公共卫生补贴的份额。
本研究使用了第四次国家家庭健康调查(NFHS-4)的数据。CS 分娩的自付费用被用作因变量,并按护理水平进行分析,即初级(PHC、UHC、其他)和二级(政府/市政、农村医院)。使用描述性统计、二元逻辑回归、受益发生率分析、集中曲线和集中指数进行分析。
从公共卫生设施使用 CS 分娩的情况来看,存在强烈的经济梯度。在使用任何公共卫生设施的母亲中,最富裕的五分之一中有 23%的人没有支付 CS 分娩费用,而最贫穷的五分之一中有 13%的人没有支付 CS 分娩费用。在使用任何类型的公共卫生设施进行 CS 分娩的母亲中,使用公共补贴具有亲富性质;最贫穷的五分之一中有 9%,较贫穷的五分之一中有 16.1%,中等的五分之一中有 24.5%,较富裕的五分之一中有 27.5%,最富裕的五分之一中有 23%。公共补贴的利用和分配模式在初级和二级卫生设施中相似,但幅度不同。受益发生率分析的结果得到了不平等分析的支持。CS 的集中指数为公立卫生中心 0.124,私立卫生中心 0.291。公立卫生中心 CS 分娩使用率的不平等程度最高的是米佐拉姆邦(0.436),其次是阿萨姆邦(0.336),最低的是泰米尔纳德邦(0.060),其次是喀拉拉邦(0.066)。
印度公立卫生中心 CS 服务的利用情况是亲富的。定期监测和评估 CS 分娩的现金激励计划,并提高贫困人口的认识,将增加公立卫生中心 CS 分娩服务的使用,并减少印度 CS 分娩的不平等。