Department of Radiation Oncology, Amsterdam UMC Location University of Amsterdam, Meibergdreef 9, Amsterdam, The Netherlands.
Department of Anesthesiology, Amsterdam UMC Location University of Amsterdam, Meibergdreef 9, Amsterdam, The Netherlands.
Radiat Oncol. 2022 May 21;17(1):99. doi: 10.1186/s13014-022-02068-5.
Due to respiratory motion, accurate radiotherapy delivery to thoracic and abdominal tumors is challenging. We aimed to quantify the ability of mechanical ventilation to reduce respiratory motion, by measuring diaphragm motion magnitudes in the same volunteers during free breathing (FB), mechanically regularized breathing (RB) at 22 breaths per minute (brpm), variation in mean diaphragm position across multiple deep inspiration breath-holds (DIBH) and diaphragm drift during single prolonged breath-holds (PBH) in two MRI sessions.
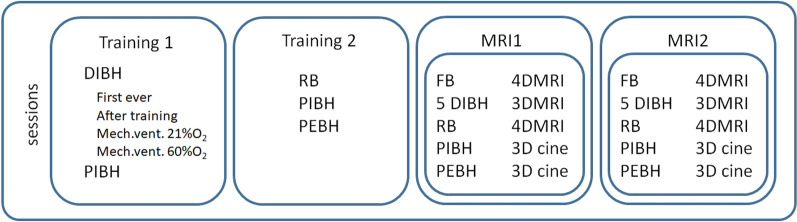
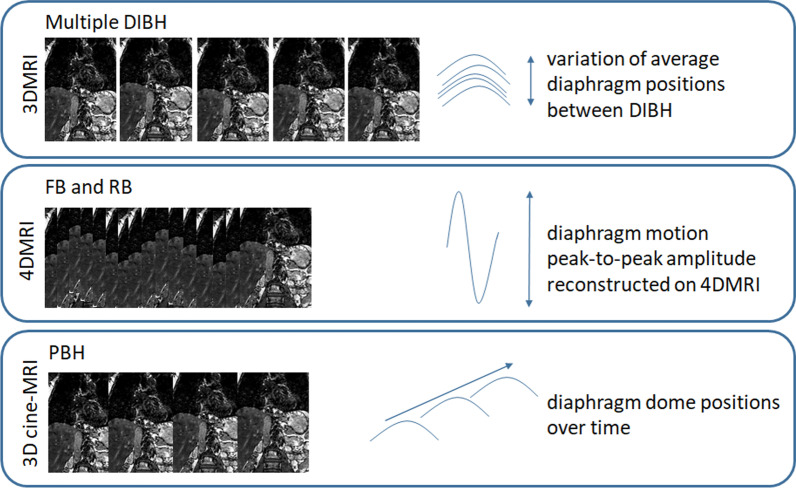
In two sessions, MRIs were acquired from fifteen healthy volunteers who were trained to be mechanically ventilated non-invasively We measured diaphragm motion amplitudes during FB and RB, the inter-quartile range (IQR) of the variation in average diaphragm position from one measurement over five consecutive DIBHs, and diaphragm cranial drift velocities during single PBHs from inhalation (PIBH) and exhalation (PEBH) breath-holds.
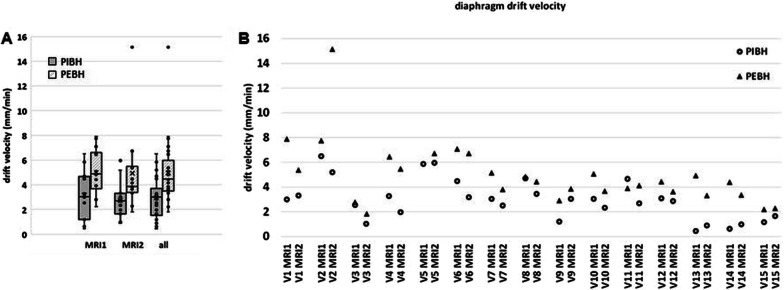
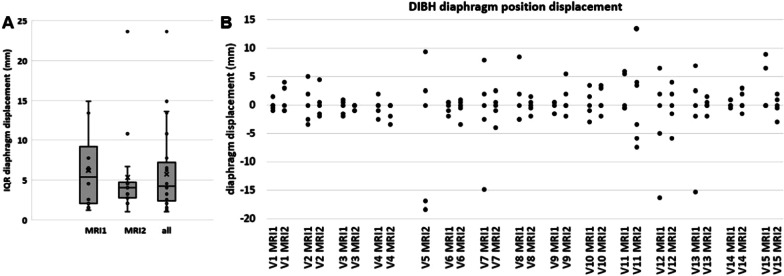
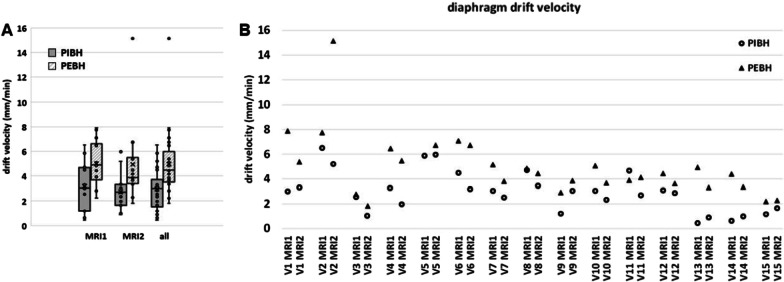
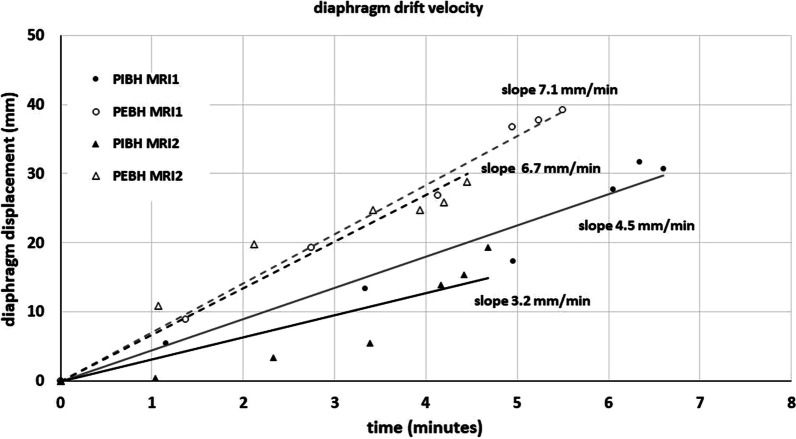
RB significantly reduced the respiratory motion amplitude by 39%, from median (range) 20.9 (10.6-41.9) mm during FB to 12.8 (6.2-23.8) mm. The median IQR for variation in average diaphragm position over multiple DIBHs was 4.2 (1.0-23.6) mm. During single PIBHs with a median duration of 7.1 (2.0-11.1) minutes, the median diaphragm cranial drift velocity was 3.0 (0.4-6.5) mm/minute. For PEBH, the median duration was 5.8 (1.8-10.2) minutes with 4.4 (1.8-15.1) mm/minute diaphragm drift velocity.
Regularized breathing at a frequency of 22 brpm resulted in significantly smaller diaphragm motion amplitudes compared to free breathing. This would enable smaller treatment volumes in radiotherapy. Furthermore, prolonged breath-holding from inhalation and exhalation with median durations of six to seven minutes are feasible.
Medical Ethics Committee protocol NL.64693.018.18.
由于呼吸运动,精确的胸腹部肿瘤放射治疗具有挑战性。我们旨在通过在两次 MRI 会话中测量相同志愿者在自由呼吸(FB)、每分钟 22 次机械规则呼吸(RB)、多次深呼吸屏气(DIBH)过程中平均膈肌位置变化的中值以及单次长时间屏气(PBH)期间膈肌漂移过程中的膈肌运动幅度,来量化机械通气减少呼吸运动的能力。
在两次会话中,从十五名经过机械通气训练的健康志愿者中获取 MRI 数据。我们测量了 FB 和 RB 期间的膈肌运动幅度、五次连续 DIBH 中平均膈肌位置变化的四分位距(IQR)以及从吸气(PIBH)和呼气(PEBH)屏气的单次 PBH 期间的膈肌颅侧漂移速度。
RB 显著降低了 39%的呼吸运动幅度,从中位数(范围)FB 期间的 20.9(10.6-41.9)mm 降至 12.8(6.2-23.8)mm。五次连续 DIBH 中平均膈肌位置变化的中值 IQR 为 4.2(1.0-23.6)mm。在中位数持续时间为 7.1(2.0-11.1)分钟的单次 PIBH 期间,中值膈肌颅侧漂移速度为 3.0(0.4-6.5)mm/min。对于 PEBH,中位数持续时间为 5.8(1.8-10.2)分钟,膈肌漂移速度为 4.4(1.8-15.1)mm/min。
与自由呼吸相比,22 次/分钟的规则呼吸导致膈肌运动幅度明显减小。这将使放射治疗的治疗体积更小。此外,从中位数持续时间为六到七分钟的吸气和呼气进行长时间屏气是可行的。
医学伦理委员会 NL.64693.018.18 号协议。