Blondon Marc, Cereghetti Sara, Pugin Jérôme, Marti Christophe, Darbellay Farhoumand Pauline, Reny Jean-Luc, Calmy Alexandra, Combescure Christophe, Mazzolai Lucia, Pantet Olivier, Ltaief Zied, Méan Marie, Manzocchi Besson Sara, Jeanneret Séverin, Stricker Hans, Robert-Ebadi Helia, Fontana Pierre, Righini Marc, Casini Alessandro
Division of Angiology and Hemostasis Geneva University Hospitals and Faculty of Medicine Geneva Switzerland.
Division of Intensive Care Geneva University Hospitals and Faculty of Medicine Geneva Switzerland.
Res Pract Thromb Haemost. 2022 May 18;6(4):e12712. doi: 10.1002/rth2.12712. eCollection 2022 May.
Hospitalized patients with COVID-19 suffered initially from high rates of venous thromboembolism (VTE), with possible associations between therapeutic anticoagulation and better clinical outcomes in observational studies.
To test whether therapeutic anticoagulation improves clinical outcomes in severe COVID-19.
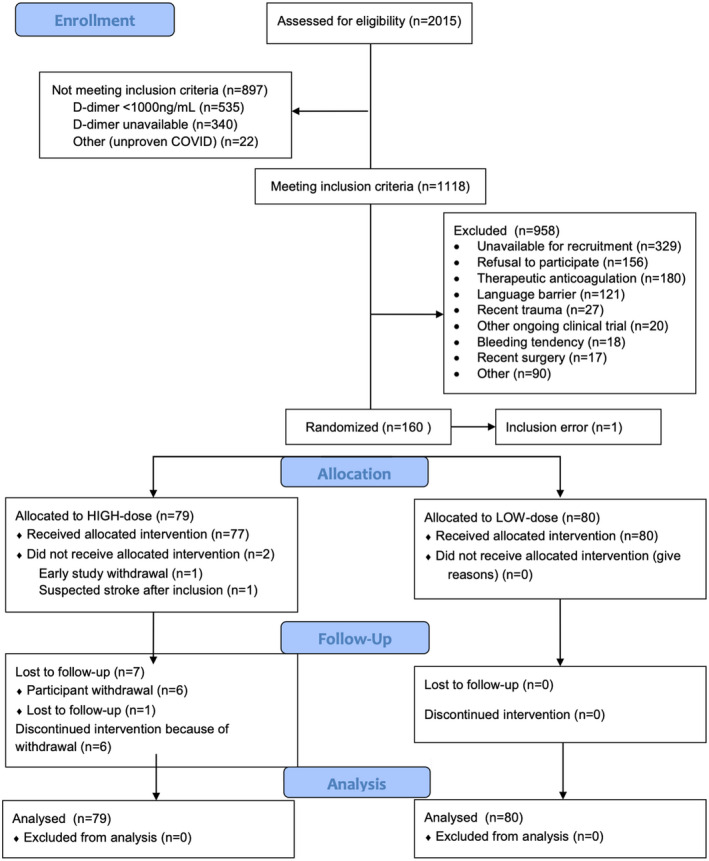
PATIENTS/METHODS: In this multicenter, open-label, randomized controlled trial, we recruited acutely ill medical COVID-19 patients with D-dimer >1000 ng/ml or critically ill COVID-19 patients in four Swiss hospitals, from April 2020 until June 2021, with a 30-day follow-up. Participants were randomized to in-hospital therapeutic anticoagulation versus low-dose anticoagulation in acutely ill participants/intermediate-dose anticoagulation in critically ill participants, with enoxaparin or unfractionated heparins. The primary outcome was a centrally adjudicated composite of 30-day all-cause mortality, VTE, arterial thrombosis, and disseminated intravascular coagulopathy (DIC), with screening for proximal deep vein thrombosis.
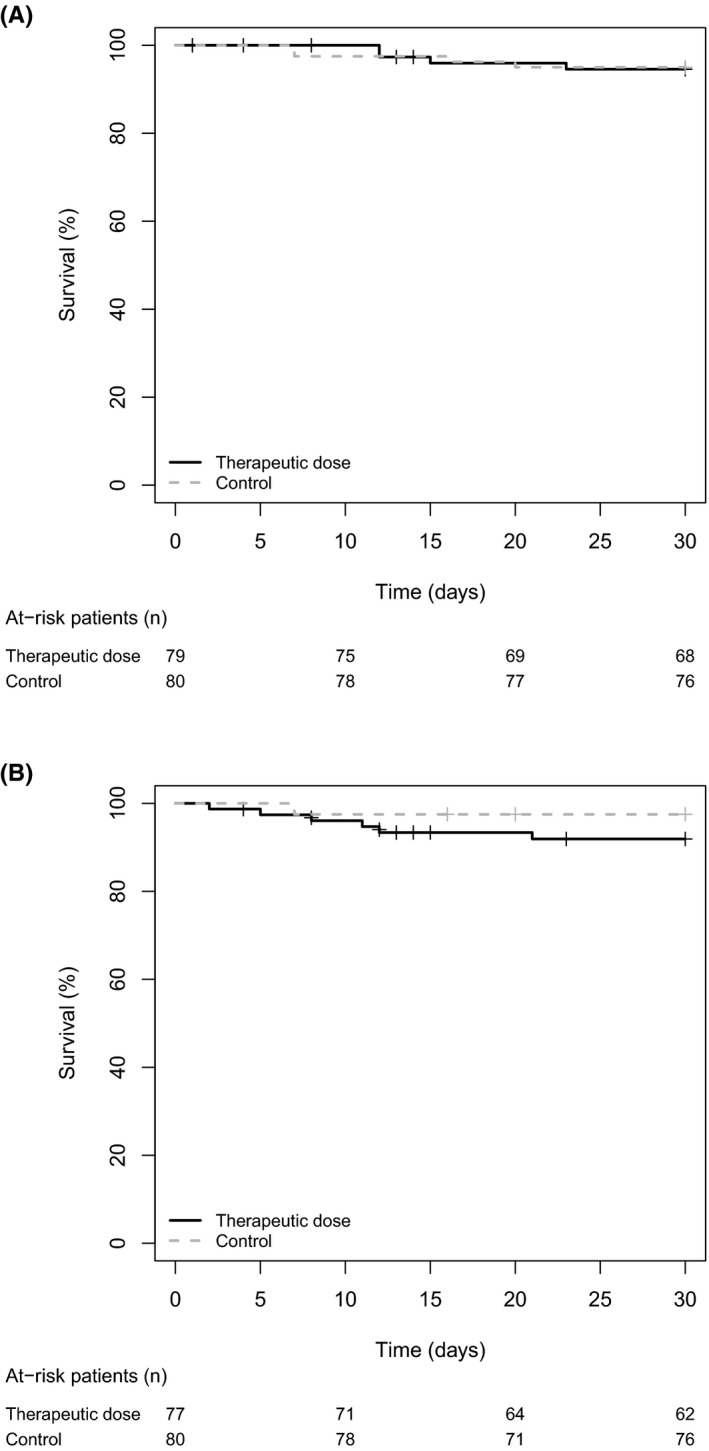
Among 159 participants, 55.3% were critically ill and 94.3% received corticosteroids. Before study inclusion, pulmonary embolism had been excluded in 71.7%. The primary outcome occurred in 4/79 participants randomized to therapeutic anticoagulation and 4/80 to low/intermediate anticoagulation (5.4% vs. 5.0%; risk difference +0.4%; adjusted hazard ratio 0.76, 95% confidence interval 0.18-3.21), including three deaths in each group. All primary outcomes and major bleeding ( = 3) occurred in critically ill participants. There was no asymptomatic proximal deep vein thrombosis and no difference in major bleeding.
Among patients with severe COVID-19 treated with corticosteroids and with exclusion of pulmonary embolism at hospital admission for most, risks of mortality, thrombotic outcomes, and DIC were low at 30 days. The lack of benefit of therapeutic anticoagulation was too imprecise for definite conclusions.
新冠肺炎住院患者最初静脉血栓栓塞(VTE)发生率较高,在观察性研究中,治疗性抗凝与更好的临床结局之间可能存在关联。
检验治疗性抗凝是否能改善重症新冠肺炎的临床结局。
患者/方法:在这项多中心、开放标签、随机对照试验中,我们于2020年4月至2021年6月在瑞士的四家医院招募了急性病医学新冠肺炎患者(D-二聚体>1000 ng/ml)或危重症新冠肺炎患者,并进行30天的随访。参与者被随机分为住院治疗性抗凝组与急性病参与者低剂量抗凝组/危重症参与者中剂量抗凝组,使用依诺肝素或普通肝素。主要结局是经中心判定的30天全因死亡率、VTE、动脉血栓形成和弥散性血管内凝血(DIC)的综合指标,并筛查近端深静脉血栓形成。
159名参与者中,55.3%为危重症,94.3%接受了皮质类固醇治疗。在纳入研究前,71.7%的患者已排除肺栓塞。随机接受治疗性抗凝的79名参与者中有4人出现主要结局,随机接受低/中剂量抗凝的80名参与者中有4人出现主要结局(5.4%对5.0%;风险差异+0.4%;调整后风险比0.76,95%置信区间0.18 - 3.21),每组各有3例死亡。所有主要结局和大出血(=3)均发生在危重症参与者中。未出现无症状近端深静脉血栓形成,大出血方面也无差异。
在大多数入院时已排除肺栓塞且接受皮质类固醇治疗的重症新冠肺炎患者中,30天时的死亡率、血栓形成结局和DIC风险较低。治疗性抗凝缺乏获益的情况不够明确,无法得出确切结论。