Yong Loo Lin School of Medicine, National University of Singapore, National University Health System, Singapore, Singapore.
Cardiothoracic Intensive Care Unit, National University Heart Centre, National University Hospital, National University Health System, Level 9, 1E Kent Ridge Road, Singapore, Singapore, 119228.
Crit Care. 2022 May 23;26(1):147. doi: 10.1186/s13054-022-04011-2.
Extracorporeal membrane oxygenation (ECMO) has been used extensively for coronavirus disease 2019 (COVID-19)-related acute respiratory distress syndrome (ARDS). Reports early in the pandemic suggested that mortality in patients with COVID-19 receiving ECMO was comparable to non-COVID-19-related ARDS. However, subsequent reports suggested that mortality appeared to be increasing over time. Therefore, we conducted an updated systematic review and meta-analysis, to characterise changes in mortality over time and elucidate risk factors for poor outcomes.
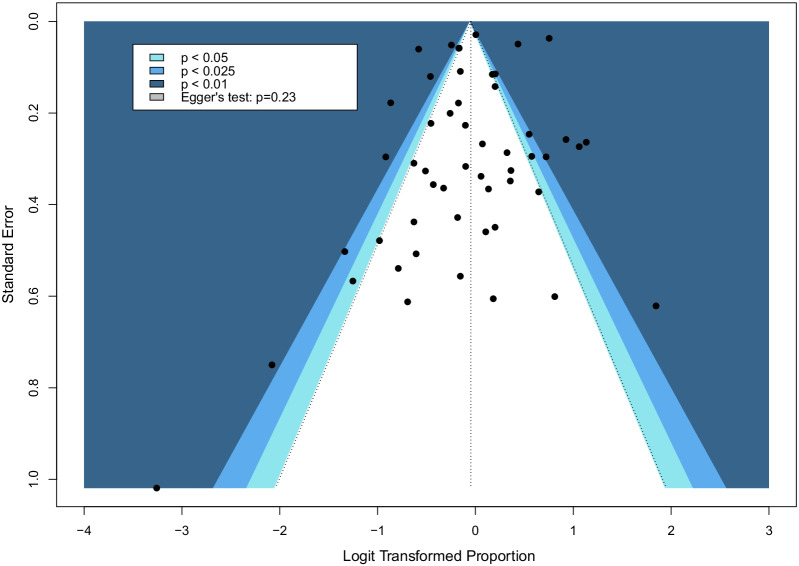
We conducted a meta-analysis (CRD42021271202), searching MEDLINE, Embase, Cochrane, and Scopus databases, from 1 December 2019 to 26 January 2022, for studies reporting on mortality among adults with COVID-19 receiving ECMO. We also captured hospital and intensive care unit lengths of stay, duration of mechanical ventilation and ECMO, as well as complications of ECMO. We conducted random-effects meta-analyses, assessed risk of bias of included studies using the Joanna Briggs Institute checklist and evaluated certainty of pooled estimates using GRADE methodology.
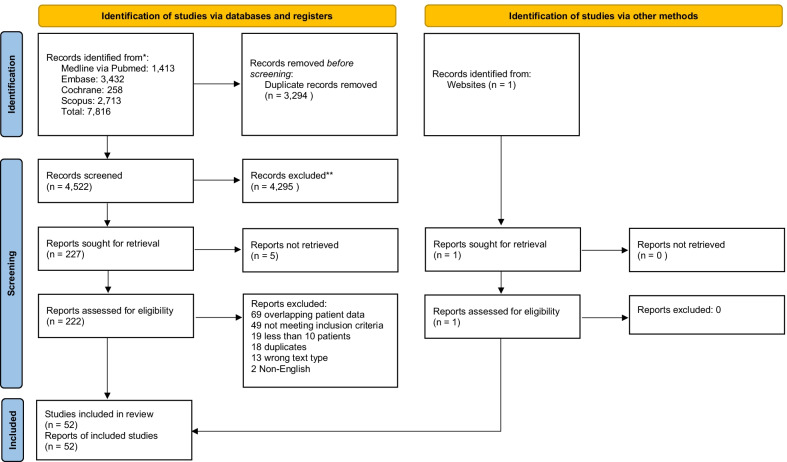
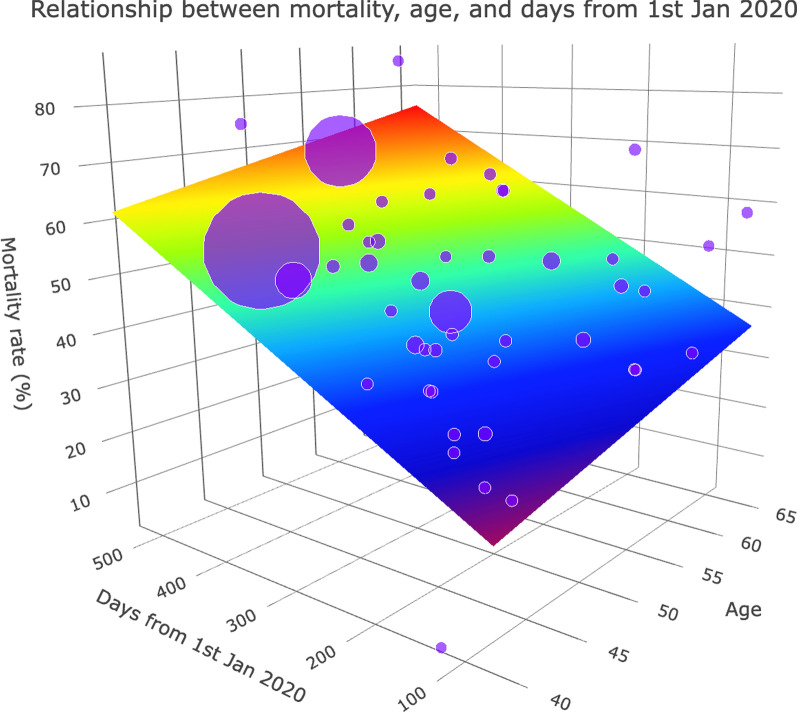
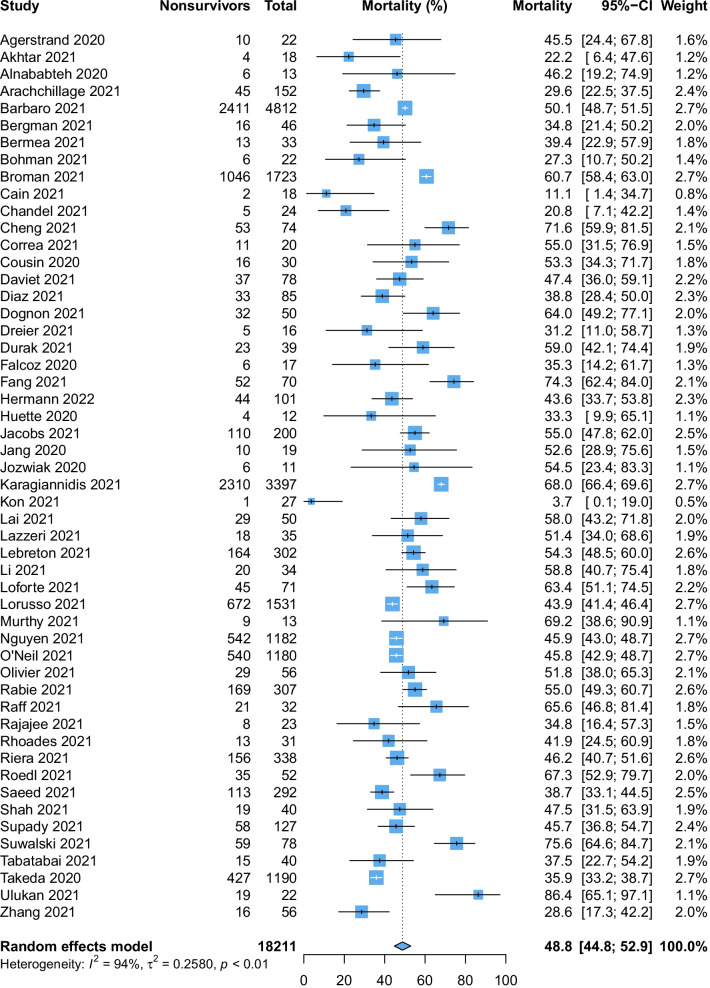
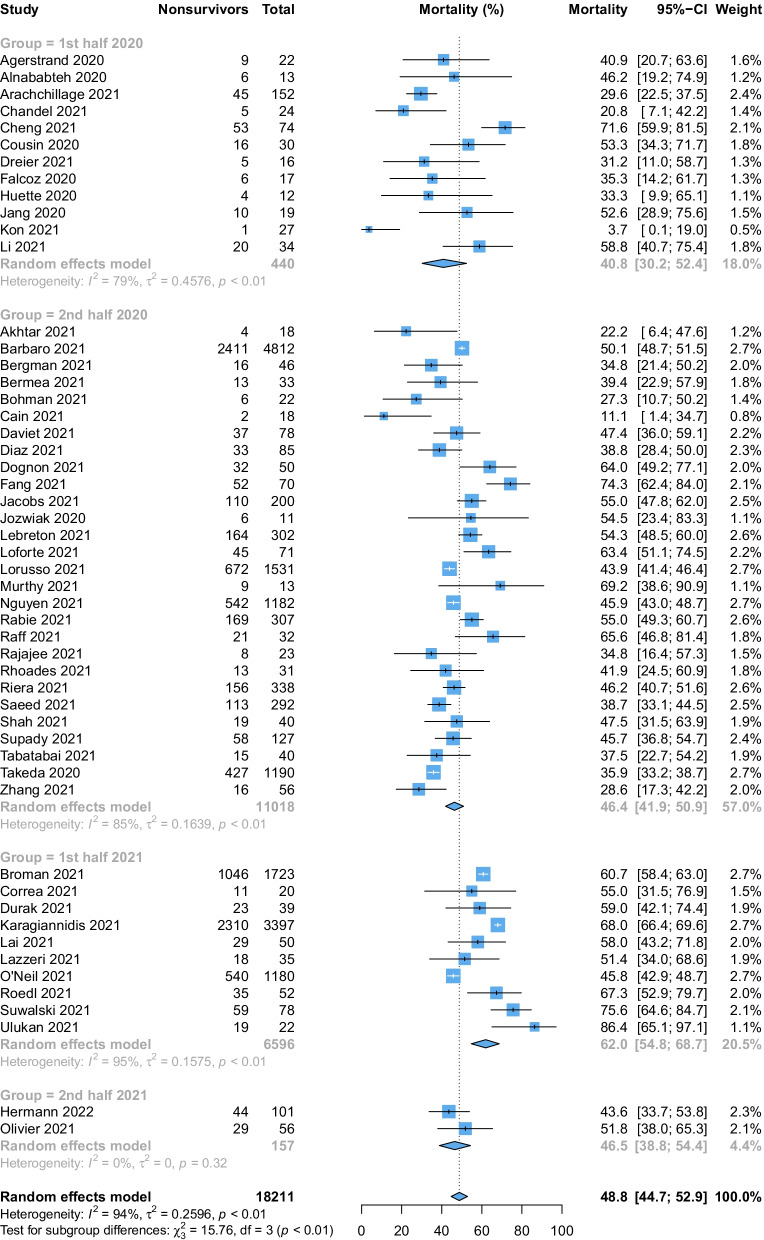
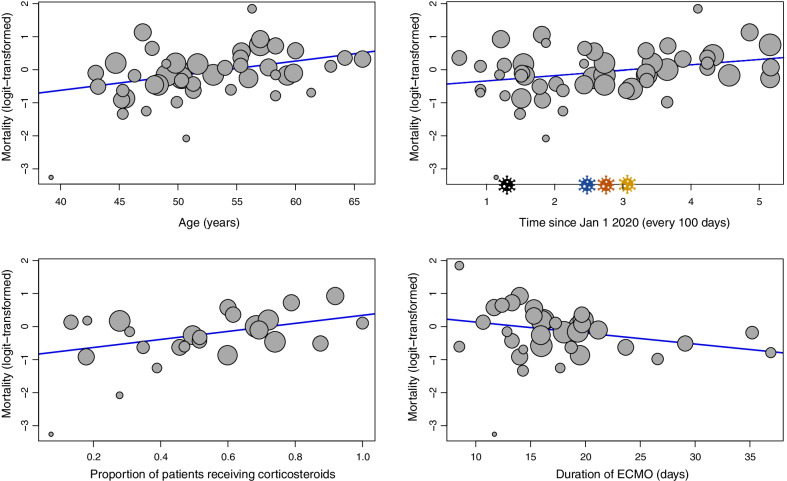
Of 4522 citations, we included 52 studies comprising 18,211 patients in the meta-analysis. The pooled mortality rate among patients with COVID-19 requiring ECMO was 48.8% (95% confidence interval 44.8-52.9%, high certainty). Mortality was higher among studies which enrolled patients later in the pandemic as opposed to earlier (1st half 2020: 41.2%, 2nd half 2020: 46.4%, 1st half 2021: 62.0%, 2nd half 2021: 46.5%, interaction p value = 0.0014). Predictors of increased mortality included age, the time of final patient enrolment from 1 January 2020, and the proportion of patients receiving corticosteroids, and reduced duration of ECMO run.
The mortality rate for patients receiving ECMO for COVID-19-related ARDS has increased as the pandemic has progressed. The reasons for this are likely multifactorial; however, as outcomes for these patients evolve, the decision to initiate ECMO should include the best contextual estimate of mortality at the time of ECMO initiation.
体外膜肺氧合(ECMO)已广泛应用于与 2019 年冠状病毒病(COVID-19)相关的急性呼吸窘迫综合征(ARDS)。大流行早期的报告表明,接受 ECMO 治疗的 COVID-19 患者的死亡率与非 COVID-19 相关的 ARDS 相当。然而,随后的报告表明,死亡率似乎随着时间的推移而增加。因此,我们进行了一项更新的系统评价和荟萃分析,以描述随时间推移死亡率的变化,并阐明不良结局的危险因素。
我们进行了荟萃分析(CRD42021271202),搜索了 MEDLINE、Embase、Cochrane 和 Scopus 数据库,从 2019 年 12 月 1 日至 2022 年 1 月 26 日,以获取报告 COVID-19 患者接受 ECMO 治疗后死亡率的研究。我们还捕获了医院和重症监护病房的住院时间、机械通气和 ECMO 的持续时间以及 ECMO 的并发症。我们进行了随机效应荟萃分析,使用 Joanna Briggs 研究所检查表评估纳入研究的偏倚风险,并使用 GRADE 方法评估汇总估计的确定性。
在 4522 条引文,我们纳入了 52 项研究,其中包括 18211 名患者的荟萃分析。需要 ECMO 的 COVID-19 患者的死亡率为 48.8%(95%置信区间 44.8-52.9%,高确定性)。与较早(2020 年上半年:41.2%,2020 年下半年:46.4%,2021 年上半年:62.0%,2021 年下半年:46.5%)相比,在大流行后期入组患者的研究中死亡率更高(交互 p 值=0.0014)。死亡率增加的预测因素包括年龄、从 2020 年 1 月 1 日最后一次患者入组的时间,以及接受皮质类固醇治疗的患者比例,以及 ECMO 运行时间缩短。
随着大流行的进展,COVID-19 相关 ARDS 患者接受 ECMO 的死亡率有所增加。原因可能是多方面的;然而,随着这些患者的结局演变,在启动 ECMO 时,应将启动 ECMO 时对死亡率的最佳背景估计纳入其中。