Haematology Department, Concord Repatriation General Hospital, Sydney, New South Wales, Australia.
Concord Clinical School, Faculty of Medicine and Health, The University of Sydney, Sydney, New South Wales, Australia.
Am J Hematol. 2023 Jan;98(1):131-139. doi: 10.1002/ajh.26619. Epub 2022 Jun 9.
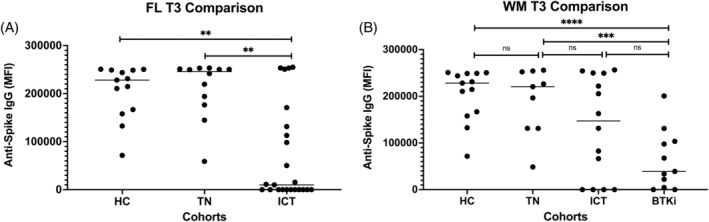
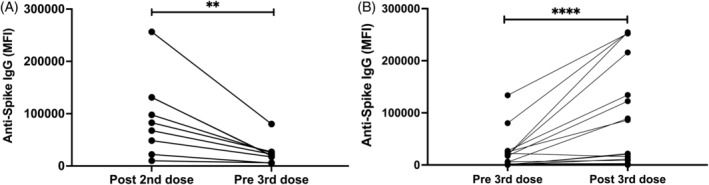
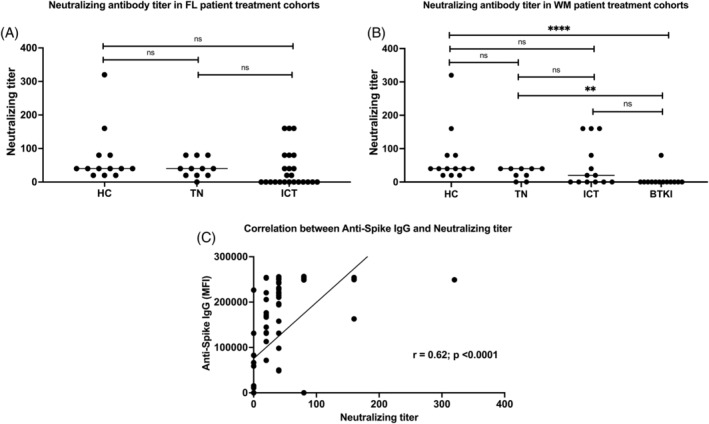
Patients with indolent lymphoma undertaking recurrent or continuous B cell suppression are at risk of severe COVID-19. Patients and healthy controls (HC; N = 13) received two doses of BNT162b2: follicular lymphoma (FL; N = 35) who were treatment naïve (TN; N = 11) or received immunochemotherapy (ICT; N = 23) and Waldenström's macroglobulinemia (WM; N = 37) including TN (N = 9), ICT (N = 14), or treated with Bruton's tyrosine kinase inhibitors (BTKi; N = 12). Anti-spike immunoglobulin G (IgG) was determined by a high-sensitivity flow-cytometric assay, in addition to live-virus neutralization. Antigen-specific T cells were identified by coexpression of CD69/CD137 and CD25/CD134 on T cells. A subgroup (N = 29) were assessed for third mRNA vaccine response, including omicron neutralization. One month after second BNT162b2, median anti-spike IgG mean fluorescence intensity (MFI) in FL ICT patients (9977) was 25-fold lower than TN (245 898) and HC (228 255, p = .0002 for both). Anti-spike IgG correlated with lymphocyte count (r = .63; p = .002), and time from treatment (r = .56; p = .007), on univariate analysis, but only with lymphocyte count on multivariate analysis (p = .03). In the WM cohort, median anti-spike IgG MFI in BTKi patients (39 039) was reduced compared to TN (220 645, p = .0008) and HC (p < .0001). Anti-spike IgG correlated with neutralization of the delta variant (r = .62, p < .0001). Median neutralization titer for WM BTKi (0) was lower than HC (40, p < .0001) for early-clade and delta. All cohorts had functional T cell responses. Median anti-spike IgG decreased 4-fold from second to third dose (p = .004). Only 5 of 29 poor initial responders assessed after third vaccination demonstrated seroconversion and improvement in neutralization activity, including to the omicron variant.
接受复发性或持续性 B 细胞抑制的惰性淋巴瘤患者有发生严重 COVID-19 的风险。患者和健康对照者(HC;N=13)接受了两剂 BNT162b2:滤泡性淋巴瘤(FL;N=35),其中包括未经治疗的患者(TN;N=11)或接受免疫化疗(ICT;N=23)和华氏巨球蛋白血症(WM;N=37),包括未经治疗的患者(N=9)、接受免疫化疗的患者(N=14)或接受布鲁顿酪氨酸激酶抑制剂(BTKi;N=12)治疗的患者。通过高灵敏度流式细胞术测定抗刺突免疫球蛋白 G(IgG),此外还测定活病毒中和作用。通过 T 细胞上共表达 CD69/CD137 和 CD25/CD134 来鉴定抗原特异性 T 细胞。亚组(N=29)评估了第三次 mRNA 疫苗应答,包括针对奥密克戎的中和作用。在第二次 BNT162b2 接种一个月后,FL ICT 患者的抗刺突 IgG 平均荧光强度(MFI)中位数(9977)比 TN(245898)和 HC(228255)低 25 倍(两者均 p=0.0002)。在单变量分析中,抗刺突 IgG 与淋巴细胞计数(r=0.63;p=0.002)和治疗时间(r=0.56;p=0.007)相关,但在多变量分析中仅与淋巴细胞计数相关(p=0.03)。在 WM 队列中,与 TN(220645,p=0.0008)和 HC(p<0.0001)相比,BTKi 患者的抗刺突 IgG MFI 中位数(39039)降低。抗刺突 IgG 与 delta 变异体的中和作用呈正相关(r=0.62,p<0.0001)。WM BTKi 的中和效价中位数(0)低于 HC(40,p<0.0001),用于早期谱系和 delta。所有队列均具有功能性 T 细胞应答。与第二次剂量相比,第三次剂量的抗刺突 IgG 中位数降低了 4 倍(p=0.004)。在第三次接种后评估的 29 名初始反应不佳的患者中,只有 5 名患者出现血清转化并提高了中和活性,包括对奥密克戎变体的中和活性。