Mielke Dorothee, Döring Katja, Behme Daniel, Psychogios Marios Nikos, Rohde Veit, Malinova Vesna
Department of Neurosurgery, Georg-August-University Göttingen, Göttingen, Germany.
Department of Neuroradiology, Georg-August-University Göttingen, Göttingen, Germany.
Front Neurol. 2022 May 9;13:838456. doi: 10.3389/fneur.2022.838456. eCollection 2022.
Cerebral vasospasm (CVS) represents one of the multiple contributors to delayed cerebral ischemia (DCI) in patients with aneurysmal subarachnoid hemorrhage (aSAH). Especially the management of CVS, refractory to medical treatment, is a challenging task during the acute phase after aSAH. Endovascular rescue therapies (ERT), such as medical and mechanical dilation, are possible treatment options on an individual basis. However, data about the influence on the patients' functional outcomes are limited. This study aims to assess the impact of ERT on the long-term functional outcome in aSAH-patients with refractory CVS.
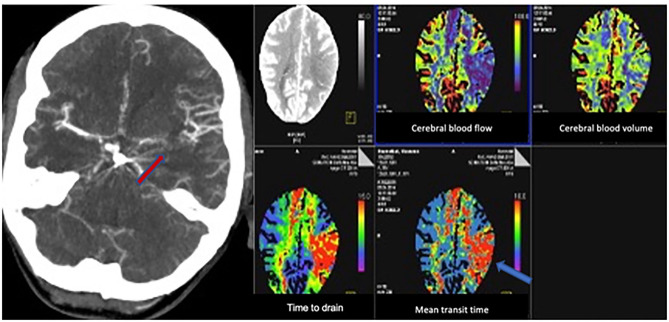
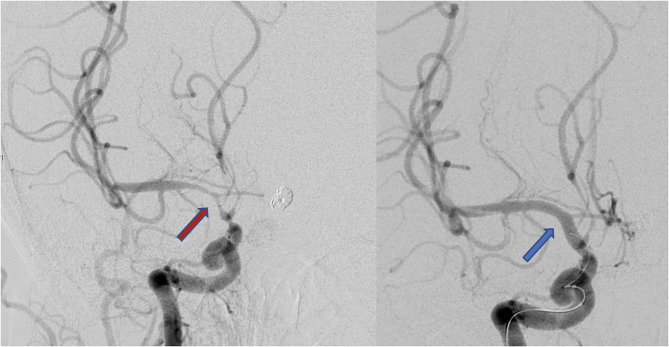
We performed a retrospective analysis of aSAH patients treated between 2012 and 2018. CVS was considered refractory, if it persisted despite oral/intravenous nimodipine application and induced hypertension. The decision to perform ETR was made on an individual basis, according to the detection of "tissue at risk" on computed tomography perfusion (CTP) scans and CVS on computed tomography angiography (CTA) or digital subtraction angiography (DSA). The functional outcome was assessed according to the modified Rankin scale (mRS) 3 months after the ictus, whereas an mRS ≤ 2 was considered as a good outcome.
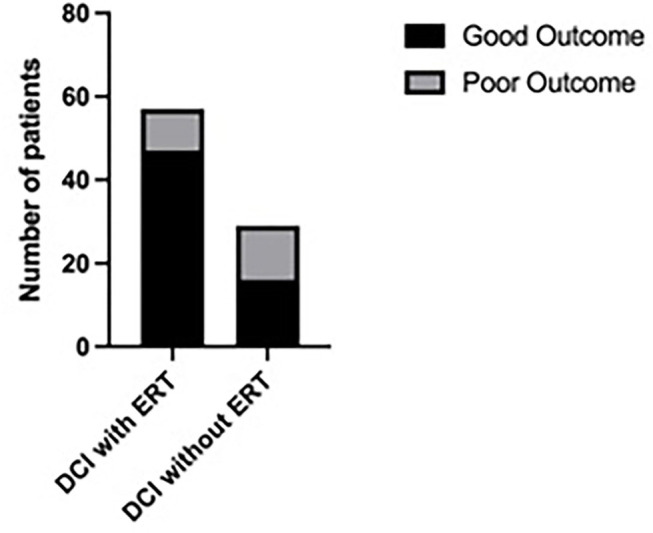
A total of 268 patients were included. Out of these, 205 patients (76.5%) were treated without ERT (group 1) and 63 patients (23.5%) with ERT (group 2). In 20 patients (31.8%) balloon dilatation was performed, in 23 patients (36.5%) intra-arterial nimodipine injection alone, and in 20 patients (31.8%) both procedures were combined. Considering only the patient group with DCI, the patients who were treated with ERT had a significantly better outcome compared to the patients without ERT (Mann-Whitney test, = 0.02).
Endovascular rescue therapies resulted in a significantly better functional outcome in patients with DCI compared to the patient group treated without ETR. CTP and CTA-based identification of "tissue at risk" might be a reliable tool for patient selection for performing ERT.
脑血管痉挛(CVS)是动脉瘤性蛛网膜下腔出血(aSAH)患者迟发性脑缺血(DCI)的多种促成因素之一。尤其是对药物治疗无效的CVS的管理,是aSAH急性期一项具有挑战性的任务。血管内抢救治疗(ERT),如药物和机械扩张,是个体化的可能治疗选择。然而,关于其对患者功能结局影响的数据有限。本研究旨在评估ERT对难治性CVS的aSAH患者长期功能结局的影响。
我们对2012年至2018年期间治疗的aSAH患者进行了回顾性分析。如果尽管应用了口服/静脉尼莫地平和诱导高血压,CVS仍持续存在,则认为其为难治性。根据计算机断层扫描灌注(CTP)扫描上“危险组织”的检测以及计算机断层扫描血管造影(CTA)或数字减影血管造影(DSA)上的CVS情况,个体化决定是否进行ERT。根据发病后3个月的改良Rankin量表(mRS)评估功能结局,mRS≤2被认为是良好结局。
共纳入268例患者。其中,205例患者(76.5%)未接受ERT治疗(第1组),63例患者(23.5%)接受ERT治疗(第2组)。20例患者(31.8%)进行了球囊扩张,23例患者(36.5%)仅进行了动脉内尼莫地平注射,20例患者(31.8%)两种操作联合进行。仅考虑患有DCI的患者组,接受ERT治疗的患者与未接受ERT治疗的患者相比,结局明显更好(曼-惠特尼检验,P = 0.02)。
与未接受ERT治疗的患者组相比,血管内抢救治疗使患有DCI的患者功能结局明显更好。基于CTP和CTA识别“危险组织”可能是选择进行ERT治疗患者的可靠工具。