Fung Kin Fen Kevin, Wong Sze Wah, Chan Eugene Yu-Hin, Cheng Ka-King, Cho Hing-Yan, Kan Elaine Yee-Ling, Ma Alison Lap Tak
Department of Radiology, Hong Kong Children's Hospital, Hong Kong, Hong Kong SAR.
Paediatric Nephrology Centre, Hong Kong Children's Hospital, Hong Kong, Hong Kong SAR.
CVIR Endovasc. 2022 May 27;5(1):24. doi: 10.1186/s42155-022-00303-4.
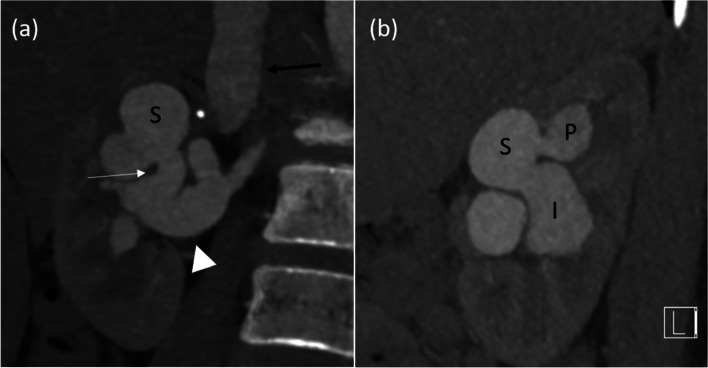
A large aneurysmal renal arteriovenous fistula (AVF) can cause hypokalaemic hypertension due to activation of renin-aldosterone system due to steal effect from renal parenchyma. In comparison to nephrectomy, endovascular embolisation of renal AVF is minimally invasive and can be nephron sparing, thus preserving renal function. However, such embolisation is technically challenging and can be associated with high risk of embolic migration.
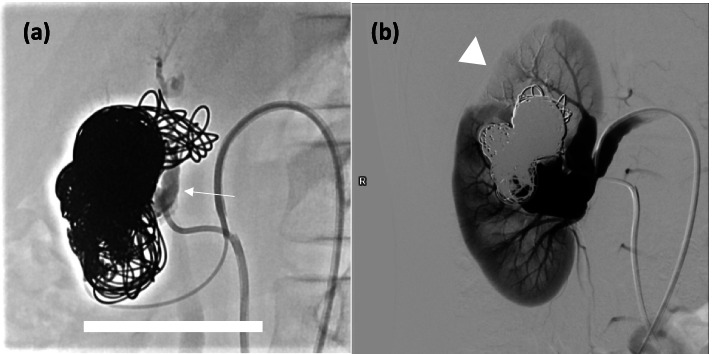
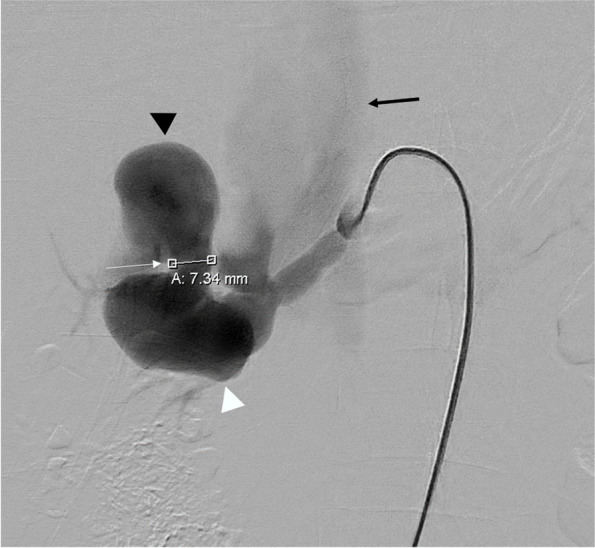
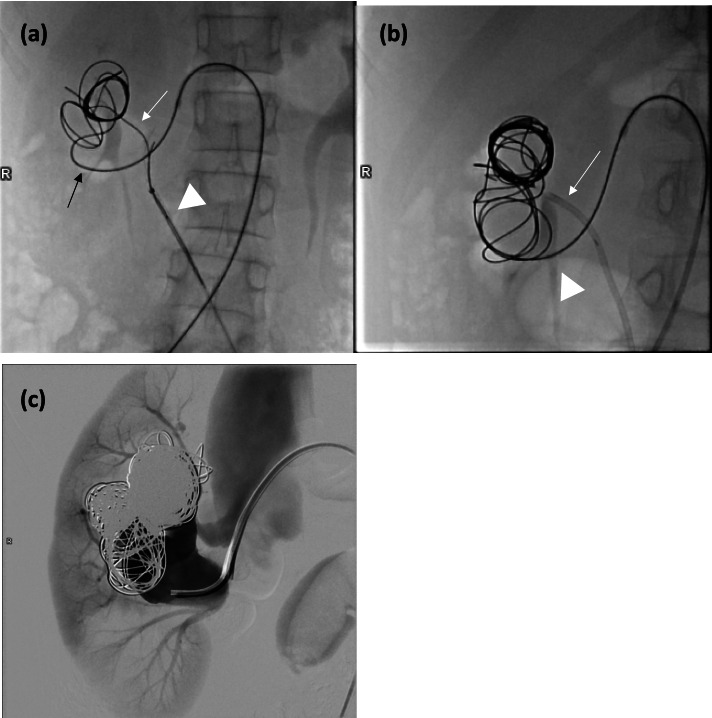
We present a case of successful embolisation of a large aneurysmal renal AVF in a 11-year-old girl. The AVF was initially treated with coil embolization via transarterial route, resulting in partial migration of coil into inferior vena cava. After removal of the migrated coil via transvenous snaring, coils were deployed simultaneously via transarterial and transvenous routes to prevent migration. AVF flow dampened but residual flow persisted at 1 month follow up. A second embolization session with additional coil deployment and N-butyl cyanoacrylate (NBCA) injection resulted in successful occlusion of the AVF. At 3 months follow up, the girl's blood pressure and serum potassium level have normalized without need of antihypertensive agent or potassium supplements.
Endovascular embolisation can be an effective nephron sparing treatment for large aneurysmal renal AVF. This is particularly important in paediatric patients as most renal function can be preserved with their expected longer life span. Risk of coil migration can be controlled by simultaneous transarterial and transvenous deployment. Complete occlusion of AVF can be aided by additional use of NBCA.
巨大的肾动静脉瘘(AVF)可因肾实质的盗血效应激活肾素 - 血管紧张素系统而导致低钾性高血压。与肾切除术相比,肾AVF的血管内栓塞是微创的,并且可以保留肾单位,从而保留肾功能。然而,这种栓塞在技术上具有挑战性,并且可能与栓塞物迁移的高风险相关。
我们报告了一例11岁女孩巨大肾AVF成功栓塞的病例。该AVF最初通过经动脉途径进行弹簧圈栓塞治疗,导致弹簧圈部分迁移至下腔静脉。通过经静脉圈套器取出迁移的弹簧圈后,同时通过经动脉和经静脉途径部署弹簧圈以防止迁移。AVF血流减弱,但在1个月随访时仍有残余血流。第二次栓塞治疗通过额外部署弹簧圈和注射N - 丁基氰基丙烯酸酯(NBCA)成功闭塞了AVF。在3个月随访时,女孩的血压和血清钾水平已恢复正常,无需使用抗高血压药物或补充钾。
血管内栓塞对于巨大肾AVF可以是一种有效的保留肾单位的治疗方法。这在儿科患者中尤为重要,因为随着预期寿命的延长,大多数肾功能可以得到保留。弹簧圈迁移的风险可以通过同时经动脉和经静脉部署来控制。额外使用NBCA有助于完全闭塞AVF。