Martínez-García María, Velasco Guillermo, Pineda Estela, Gil-Gil Miguel, Alameda Francesc, Capellades Jaume, Martín-Soberón Mari Cruz, López-Valero Israel, Tovar Ambel Elena, Foro Palmira, Taus Álvaro, Arumi Montserrat, Hernández-Laín Aurelio, Sepúlveda-Sánchez Juan Manuel
Medical Oncology Department, Hospital del Mar, 08003 Barcelona, Spain.
Medical Oncology Department, Centro Integral Oncológico Clara Campal HM Delfos, 08023 Barcelona, Spain.
Cancers (Basel). 2022 May 12;14(10):2393. doi: 10.3390/cancers14102393.
MET-signaling and midkine (ALK ligand) promote glioma cell maintenance and resistance against anticancer therapies. ALK and c-MET inhibition with crizotinib have a preclinical therapeutic rationale to be tested in newly diagnosed GBM.
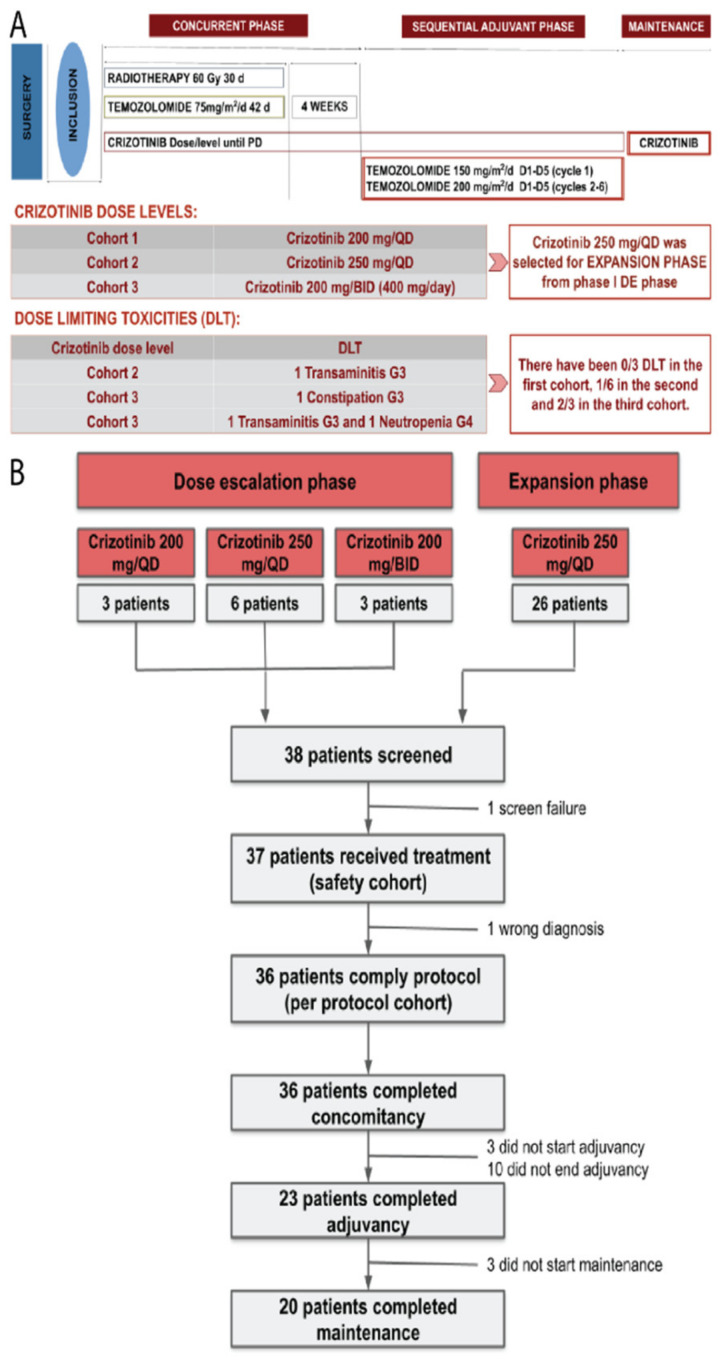
Eligible patients received crizotinib with standard radiotherapy (RT)/temozolomide (TMZ) followed by maintenance with crizotinib. The primary objective was to determine the recommended phase 2 dose (RP2D) in a 3 + 3 dose escalation (DE) strategy and safety evaluation in the expansion cohort (EC). Secondary objectives included progression-free (PFS) and overall survival (OS) and exploratory biomarker analysis.
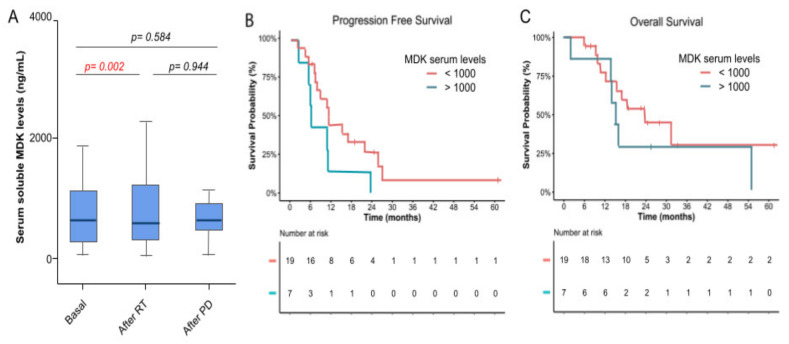
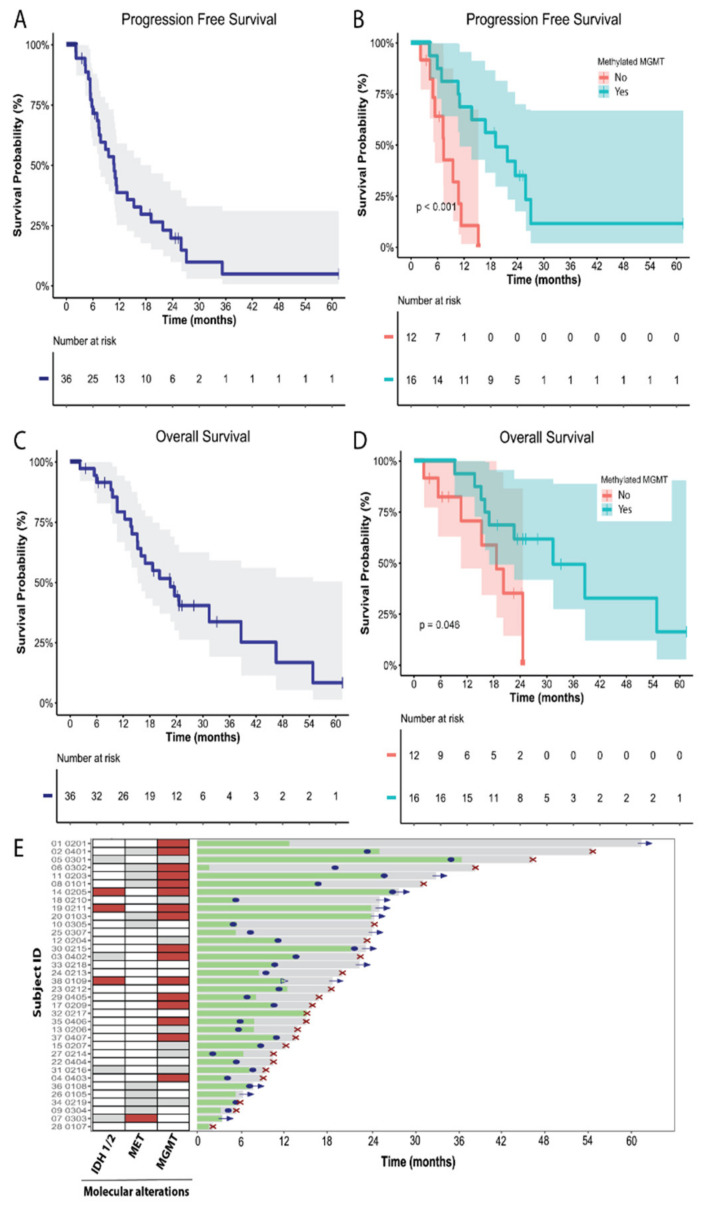
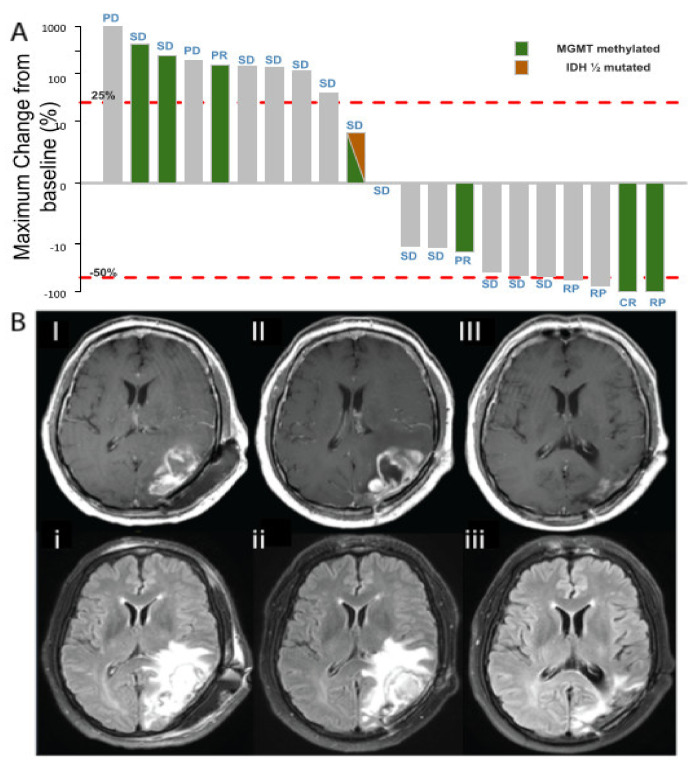
The study enrolled 38 patients. The median age was 52 years (33-76), 44% were male, 44% were MGMT methylated, and three patients had IDH1/2 mutation. In DE, DLTs were reported in 1/6 in the second cohort (250 mg/QD), declaring 250 mg/QD of crizotinib as the RP2D for the EC. In the EC, 9/25 patients (32%) presented grade ≥3 adverse events. The median follow up was 18.7 months (m) and the median PFS was 10.7 m (95% CI, 7.7-13.8), with a 6 m PFS and 12 m PFS of 71.5% and 38.8%, respectively. At the time of this analysis, 1 died without progression and 24 had progressed. The median OS was 22.6 m (95% CI, 14.1-31.1) with a 24 m OS of 44.5%. Molecular biomarkers showed no correlation with efficacy.
The addition of crizotinib to standard RT and TMZ for newly diagnosed GBM was safe and the efficacy was encouraging, warranting prospective validation in an adequately powered, randomized controlled study.
MET信号传导和中期因子(ALK配体)可促进胶质瘤细胞存活并对抗癌治疗产生耐药性。克唑替尼抑制ALK和c-MET在新诊断的胶质母细胞瘤中有临床前治疗依据待验证。
符合条件的患者接受克唑替尼联合标准放疗(RT)/替莫唑胺(TMZ)治疗,随后接受克唑替尼维持治疗。主要目的是在3+3剂量递增(DE)策略中确定推荐的2期剂量(RP2D)并在扩展队列(EC)中进行安全性评估。次要目的包括无进展生存期(PFS)和总生存期(OS)以及探索性生物标志物分析。
该研究纳入了38例患者。中位年龄为52岁(33-76岁),44%为男性,44%的患者MGMT基因甲基化,3例患者存在IDH1/2突变。在DE阶段,第二个队列(250mg/每日一次)中有1/6的患者报告了剂量限制性毒性(DLT),确定250mg/每日一次的克唑替尼为EC的RP2D。在EC中,9/25例患者(32%)出现≥3级不良事件。中位随访时间为18.7个月(m),中位PFS为10.7m(95%CI,7.7-13.8),6个月和12个月的PFS率分别为71.5%和38.8%。在本次分析时,1例患者无进展死亡,24例患者病情进展。中位OS为22.6m(95%CI,14.1-31.1),24个月的OS率为44.5%。分子生物标志物与疗效无相关性。
对于新诊断的胶质母细胞瘤,在标准RT和TMZ基础上加用克唑替尼是安全的,疗效令人鼓舞,需要在一项有足够样本量的前瞻性随机对照研究中进行验证。