Department of Internal Medicine II, University Hospital Würzburg, Würzburg, Germany.
Department of Hematology, Medical Oncology, and Pneumology, University Medical Centre of the Johannes Gutenberg University Mainz, Mainz, Germany.
Infection. 2022 Dec;50(6):1543-1555. doi: 10.1007/s15010-022-01847-2. Epub 2022 May 28.
This study aimed to describe the cytomegalovirus (CMV) infection rate, rehospitalizations, and comorbidities following allogeneic hematopoietic stem cell transplantation (allo-HSCT) and solid organ transplantation (SOT).
Patients who received allo-HSCT or SOT in 01/07/2015-30/06/2018 were identified using anonymized German claims data. The transplantation-related hospital admission date was defined as the index date, and patients were followed for up to 12 months (or death, first event relevant). The frequency of CMV infections (confirmed outpatient/inpatient diagnoses, ICD-10-GM codes: B25.-/B27.1) and the rate, number, and duration of all-cause rehospitalizations in the follow-up period were evaluated.
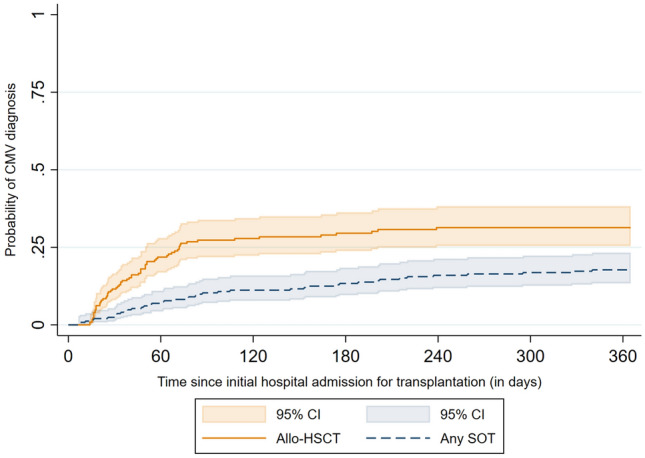
A total of 226 allo-HSCT and 250 SOT patients were identified (mean age 52.8 years, 38.9% female). During the 12 months after transplantation, 29.2% of allo-HSCT patients and 16.8% of SOT patients received a CMV diagnosis. The majority of these diagnoses were given during the initial hospitalization or within the following 3 months. Across transplantation types, CMV patients had more hospital readmission days per patient-year (allo-HSCT 93.3 vs. 49.4, p = 0.001; SOT 42.0 vs. 20.7, p = 0.005), with a longer mean duration of readmissions (allo-HSCT 22.4 vs. 15.4 days, p < 0.001; SOT 11.6 vs. 7.5 days, p = 0.003). Comorbidity burden in transplantation patients was substantial, with several diagnoses being significantly more common among patients with CMV vs. non-CMV. One-year mortality did not differ significantly between patients with/without CMV.
Burden of transplant recipients with CMV in terms of rehospitalizations and comorbidities is substantial, highlighting the need for improved CMV prevention and treatment.
本研究旨在描述异基因造血干细胞移植(allo-HSCT)和实体器官移植(SOT)后巨细胞病毒(CMV)感染率、再入院率和合并症。
使用匿名德国索赔数据确定 2015 年 7 月 1 日至 2018 年 6 月 30 日接受 allo-HSCT 或 SOT 的患者。移植相关住院日期定义为索引日期,并在随访期间最多随访 12 个月(或死亡,首次相关事件)。评估随访期间 CMV 感染的频率(经确认的门诊/住院诊断,ICD-10-GM 代码:B25.-/B27.1)以及全因再入院的发生率、数量和持续时间。
共确定了 226 例 allo-HSCT 和 250 例 SOT 患者(平均年龄 52.8 岁,38.9%为女性)。在移植后 12 个月内,29.2%的 allo-HSCT 患者和 16.8%的 SOT 患者被诊断为 CMV。这些诊断大多数是在初始住院期间或随后的 3 个月内做出的。在两种移植类型中,CMV 患者的患者年再入院天数更多(allo-HSCT 93.3 天 vs. 49.4 天,p = 0.001;SOT 42.0 天 vs. 20.7 天,p = 0.005),再入院的平均持续时间更长(allo-HSCT 22.4 天 vs. 15.4 天,p < 0.001;SOT 11.6 天 vs. 7.5 天,p = 0.003)。移植患者的合并症负担相当大,一些诊断在 CMV 患者和非 CMV 患者中的发生率显著更高。CMV 患者和非 CMV 患者的 1 年死亡率无显著差异。
CMV 感染的移植受者在再入院和合并症方面的负担相当大,这突出表明需要改进 CMV 的预防和治疗。