Hsu Jim, Annunziata Joseph F, Burns Ethan, Bernicker Eric H, Olsen Randall J, Thomas Jessica S
Department of Pathology and Genomic Medicine, Houston Methodist Hospital, Houston, TX, USA.
Clinical Pathology Associates, Norton Healthcare, Louisville, KY, USA.
Clin Pathol. 2022 May 23;15:2632010X221102054. doi: 10.1177/2632010X221102054. eCollection 2022 Jan-Dec.
mutations are the most common oncogenic driver mutations of non-small cell lung cancer (NSCLC) in the Western world. Mutations of the gene are most prevalent in the patient population of current and former cigarette smokers. With the recent pivotal approval of a targeted inhibitor therapy for patients with p.G12C mutated and pretreated NSCLC, analysis of the heterogeneity of mutations and concomitant molecular alterations in patients with these tumors at all clinical stages is indicated.
In this retrospective analysis, patient pathology records were reviewed for all cases receiving a pathologic diagnosis of NSCLC within our hospital system. All data were collected with IRB approval. Cases of indeterminate tumor type favoring a non-lung primary, as well as non-adenocarcinoma NSCLC (eg, squamous) were excluded from the cohort. In this hospital system, molecular testing for mutations is part of a molecular biomarker panel that is reflex ordered at initial diagnosis by the pathologist and may be performed as a single gene test or as a solid organ cancer hotspot panel by next generation sequencing. For each patient, mutational status and specific mutations, if present, were collated. Additional information assessed for this study included patient demographics (age, gender, and smoking history), tumor staging if available, PD-L1 expression levels by immunohistochemistry (IHC), and the presence of other genetic alterations (, , and ).
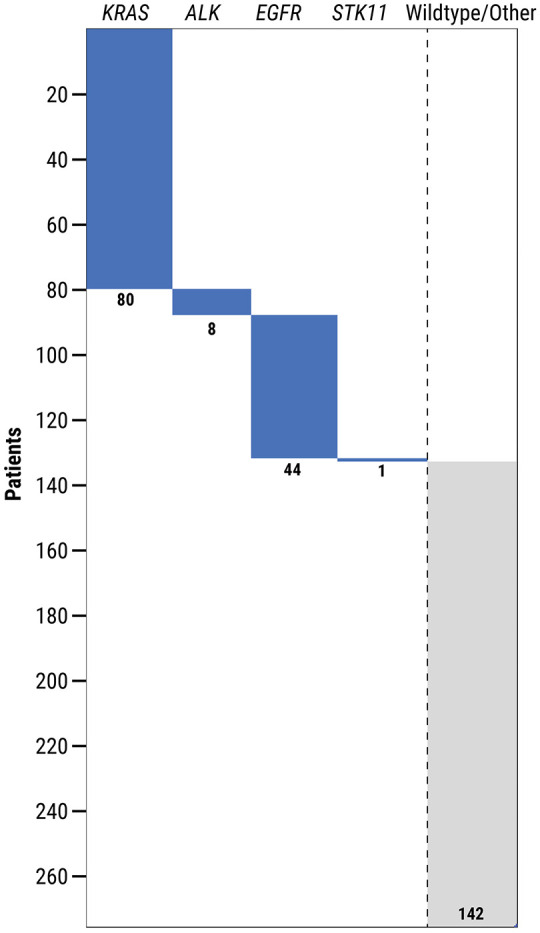
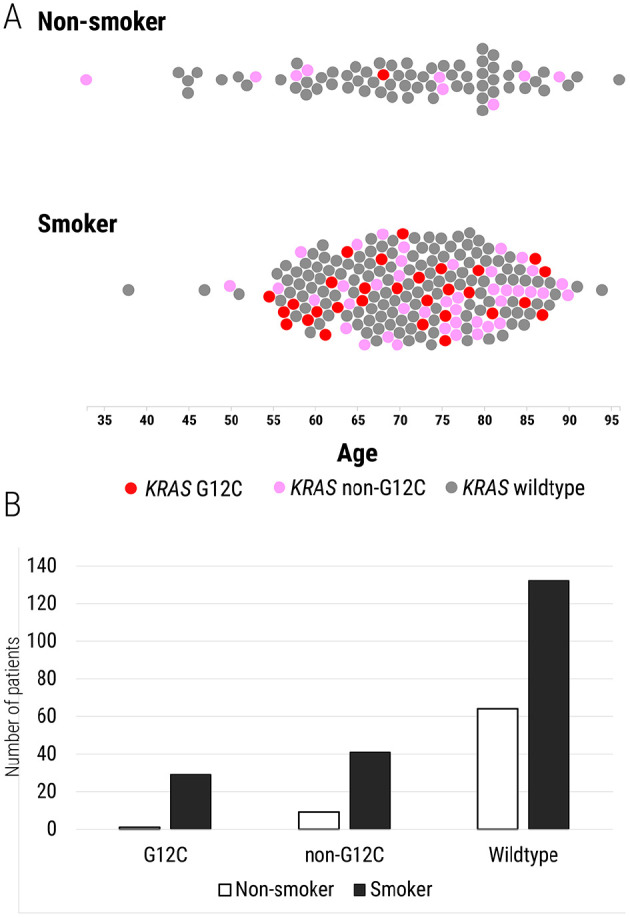
Between January 1, 2017 and January 1, 2019, there were 276 patients diagnosed with NSCLC of all stages who had mutational analysis performed in our hospital system and who met the criteria for inclusion into the study cohort. A driver mutation was detected in 29% of these patients. The most frequently identified mutation was p.G12C (38%), followed by p.G12D (21%) and p.G12V (13%). mutated lung adenocarcinoma was significantly associated with current or former patient smoking status in this cohort (29/202 (14%) smokers and 1/74 (1%) non-smokers; = .0006). PD-L1 expression of at least 1% by IHC was present in 43% of -mutated lung adenocarcinomas and 45% of non--mutated adenocarcinomas. In this study, mutations were not found to co-occur with gene alterations in , , or . In 48% of cases, at least one genetic alteration (, , , or ) was identified.
In this study cohort, -mutated lung adenocarcinoma demonstrated significant mutational heterogeneity, which is consistent with previously published studies. mutational status was also significantly associated with a current or former smoking history. Notably, p.G12C was the most frequently identified mutation in this cohort, with a frequency of 38%. This finding is particularly relevant given the recent approval of a p.G12C-specific targeted inhibitor therapy and the continued development of additional targeted therapies that may prove effective in treating NSCLC. These findings also highlight the necessity of considering molecular testing for mutations in patients with NSCLC and a smoking history, as this population most frequently harbors mutations and may benefit from these emerging targeted therapies.

在西方世界,KRAS突变是非小细胞肺癌(NSCLC)最常见的致癌驱动突变。KRAS基因的突变在当前和既往吸烟者的患者群体中最为普遍。随着针对携带p.G12C突变且经治的NSCLC患者的靶向抑制剂疗法最近获得关键批准,有必要分析这些肿瘤患者在所有临床阶段的KRAS突变异质性及伴随的分子改变。
在这项回顾性分析中,我们回顾了我院系统内所有接受NSCLC病理诊断的病例的患者病理记录。所有数据均在获得机构审查委员会(IRB)批准后收集。肿瘤类型不确定且倾向于非肺原发性肿瘤的病例,以及非腺癌NSCLC(如鳞癌)被排除在队列之外。在我院系统中,KRAS突变的分子检测是分子生物标志物检测 panel 的一部分,由病理学家在初始诊断时进行 reflex 排序,可通过下一代测序作为单基因检测或实体器官癌症热点 panel 进行。对于每位患者,整理了KRAS突变状态及特定的KRAS突变(如有)。本研究评估的其他信息包括患者人口统计学特征(年龄、性别和吸烟史)、可用的肿瘤分期、免疫组织化学(IHC)检测的PD-L1表达水平以及其他基因改变(EGFR、ALK和BRAF)的存在情况。
在2017年1月1日至2019年1月1日期间,我院系统中有276例各阶段NSCLC患者进行了KRAS突变分析,且符合纳入研究队列的标准。这些患者中有29%检测到KRAS驱动突变。最常鉴定出的KRAS突变是p.G12C(38%),其次是p.G12D(21%)和p.G12V(13%)。在该队列中,KRAS突变的肺腺癌与当前或既往患者吸烟状态显著相关(202名吸烟者中有29名(14%),74名非吸烟者中有1名(1%);P = 0.0006)。通过IHC检测,至少1%的KRAS突变肺腺癌和45%的非KRAS突变腺癌存在PD-L1表达。在本研究中,未发现KRAS突变与EGFR、ALK或BRAF基因改变同时发生。在48%的病例中,鉴定出至少一种基因改变(EGFR、ALK、BRAF或其他)。
在本研究队列中,KRAS突变的肺腺癌表现出显著的突变异质性,这与先前发表的研究一致。KRAS突变状态也与当前或既往吸烟史显著相关。值得注意的是,p.G12C是该队列中最常鉴定出的KRAS突变,频率为38%。鉴于最近p.G12C特异性靶向抑制剂疗法的批准以及可能证明对治疗NSCLC有效的其他KRAS靶向疗法的持续开发,这一发现尤为重要。这些发现还强调了在有吸烟史的NSCLC患者中考虑进行KRAS突变分子检测的必要性,因为该人群最常携带KRAS突变,可能从这些新兴的靶向疗法中获益。