Ludwig Boltzmann Institute for Cardiovascular Research at the Center for Biomedical Research, Medical University of Vienna, Vienna, Austria.
Institute of Physiology, Center for Physiology and Pharmacology, Medical University of Vienna, Vienna, Austria.
Interact Cardiovasc Thorac Surg. 2022 Jun 15;35(1). doi: 10.1093/icvts/ivac152.
We have previously demonstrated beneficial cardiac protection with hypothermic polarizing cardioplegia compared to a hyperkalemic depolarizing cardioplegia. In this study, a porcine model of cardiopulmonary bypass was used to compare the protective effects of normothermic blood-based polarizing and depolarizing cardioplegia during cardiac arrest.
Thirteen pigs were randomized to receive either normothermic polarizing (n = 8) or depolarizing (n = 5) blood-based cardioplegia. After initiation of cardiopulmonary bypass, normothermic arrest (34°C, 60 min) was followed by 60 min of on-pump and 90 min of off-pump reperfusion. Primary outcome was myocardial injury measured as arterial myocardial creatine kinase concentration. Secondary outcome was haemodynamic function and the energy state of the hearts.
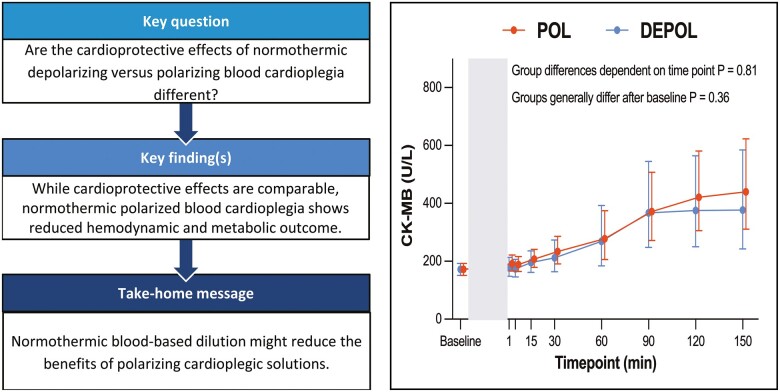
During reperfusion, release of myocardial creatine kinase was comparable between groups (P = 0.36). In addition, most haemodynamic parameters showed comparable results between groups, but stroke volume (P = 0.03) was significantly lower in the polarizing group. Adenosine triphosphate levels were significantly (18.41 ± 3.86 vs 22.97 ± 2.73 nmol/mg; P = 0.03) lower in polarizing hearts, and the requirement for noradrenaline administration (P = 0.002) and temporary pacing (6 vs 0; P = 0.02) during reperfusion were significantly higher in polarizing hearts.
Under normothermic conditions, polarizing blood cardioplegia was associated with similar myocardial injury to depolarizing blood cardioplegia. Reduced haemodynamic and metabolic outcome and a higher need for temporary pacing with polarized arrest may be associated with the blood-based dilution of this solution.
我们之前的研究表明,与高钾去极化停搏液相比,低温极化停搏液可对心脏起到有益的保护作用。在这项研究中,我们使用猪体外循环模型来比较常温血基极化和去极化停搏液在心脏停搏期间的保护作用。
将 13 头猪随机分为常温极化(n = 8)或去极化(n = 5)血基停搏液组。体外循环开始后,常温(34°C)停搏 60min,随后泵血 60min 和停泵后再灌注 90min。主要终点是动脉心肌肌酸激酶浓度评估的心肌损伤。次要终点是血流动力学功能和心脏的能量状态。
在再灌注期间,两组间心肌肌酸激酶的释放无差异(P = 0.36)。此外,大多数血流动力学参数在两组间的结果无差异,但极化组的每搏量显著降低(P = 0.03)。三磷酸腺苷水平在极化组显著降低(18.41 ± 3.86 与 22.97 ± 2.73 nmol/mg;P = 0.03),再灌注期间去甲肾上腺素的应用(P = 0.002)和临时起搏(6 次与 0 次;P = 0.02)的需求也显著增加。
在常温条件下,极化血停搏液与去极化血停搏液引起的心肌损伤相似。较低的血流动力学和代谢结果以及极化停搏时对临时起搏的较高需求可能与该溶液的血基稀释有关。