Arthroplasty Center, Helios Klinikum Munich West, Steinerweg 5, 81241, Munich, Germany.
Universitätsklinik für Orthopädie, Medizinische Universität Innsbruck, Anichstraße 35, 6020, Innsbruck, Austria.
Oper Orthop Traumatol. 2022 Jun;34(3):218-230. doi: 10.1007/s00064-022-00770-x. Epub 2022 May 31.
Proximal femoral replacement (PFR) is a salvage procedure originally developed for reconstruction after resection of sarcomas and metastatic cancer. These techniques can also be adapted for the treatment of non-oncologic reconstruction for cases involving massive proximal bone loss. The direct anterior approach (DAA) is readily utilized for revision total hip arthroplasty (THA), but there have been few reports of its use for proximal femoral replacement.
Aseptic, septic femoral implant loosening, periprosthetic femoral fracture, oncologic lesions of the proximal femur. The most common indication for non-oncologic proximal femoral placement is a severe femoral defect Paprosky IIIB or IV.
Infection.
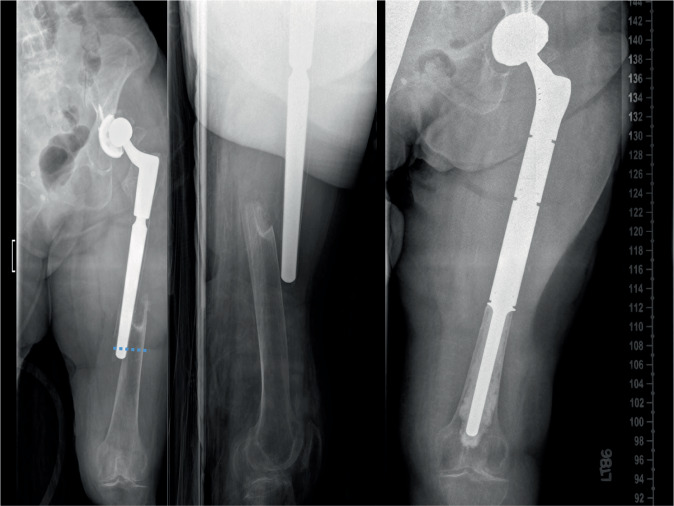
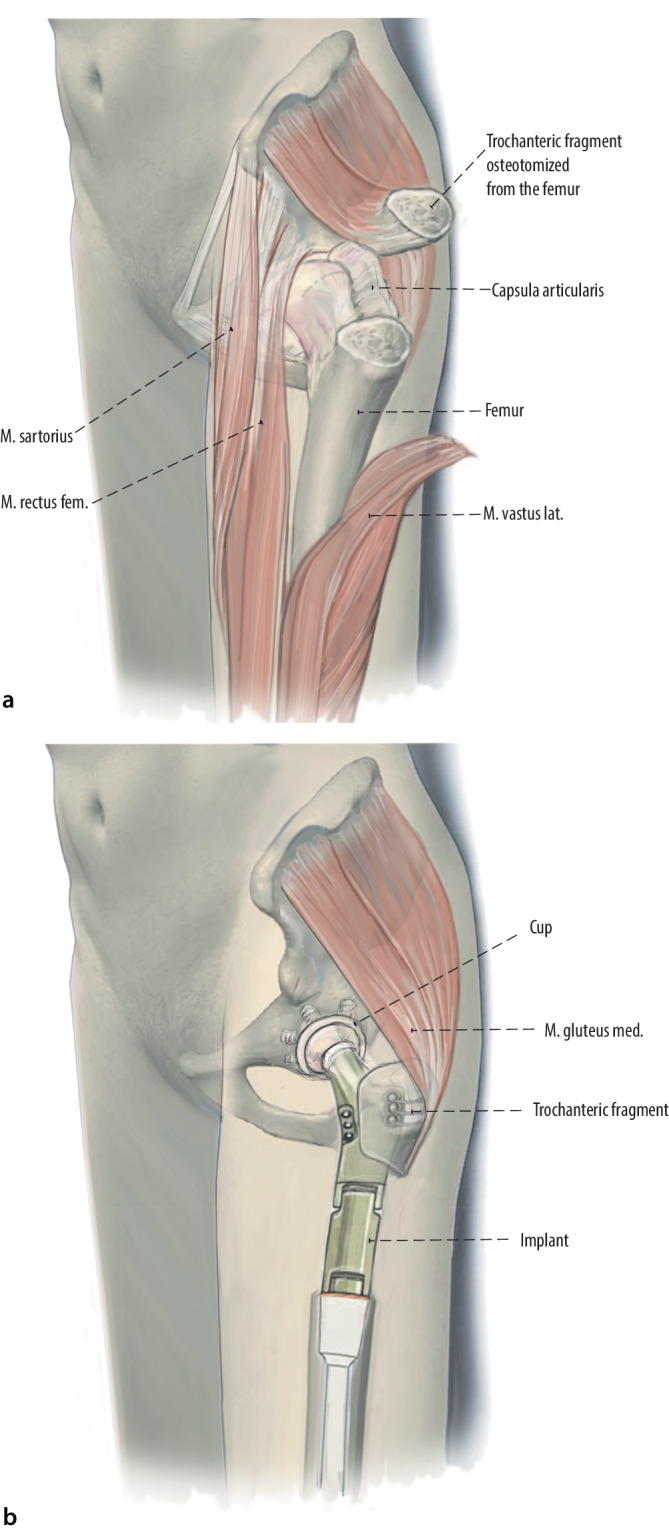
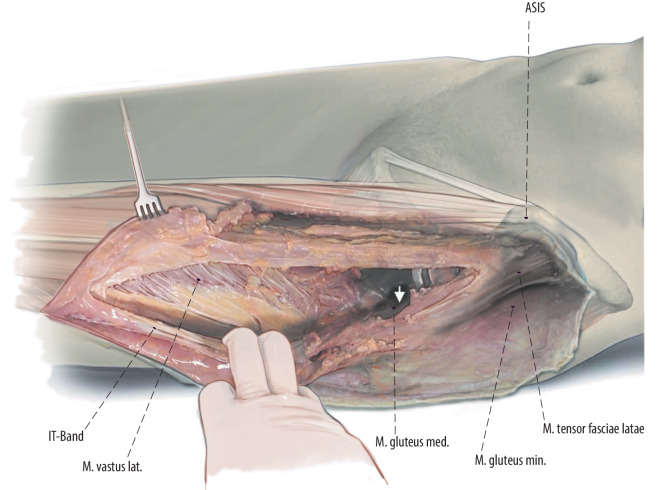
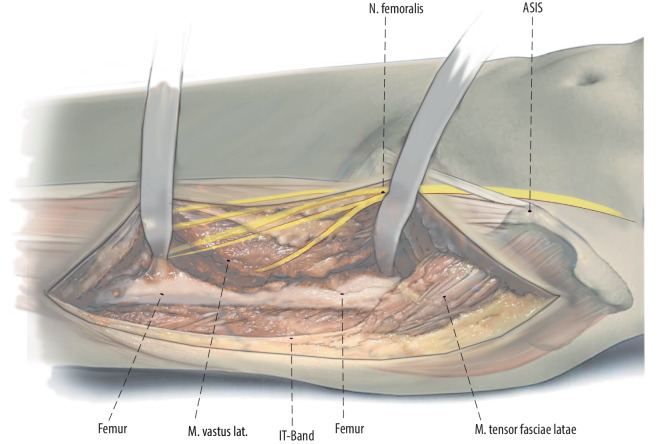
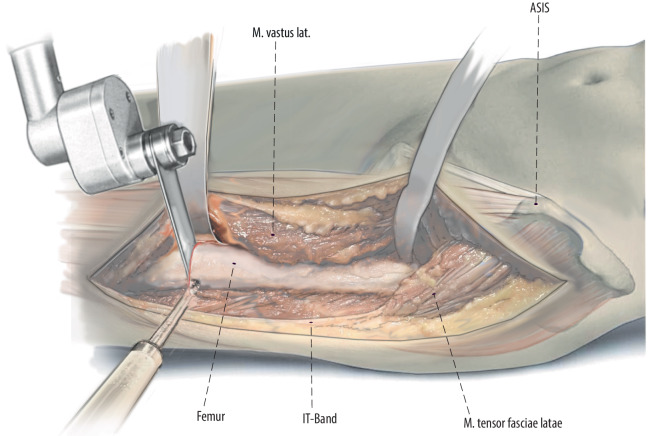
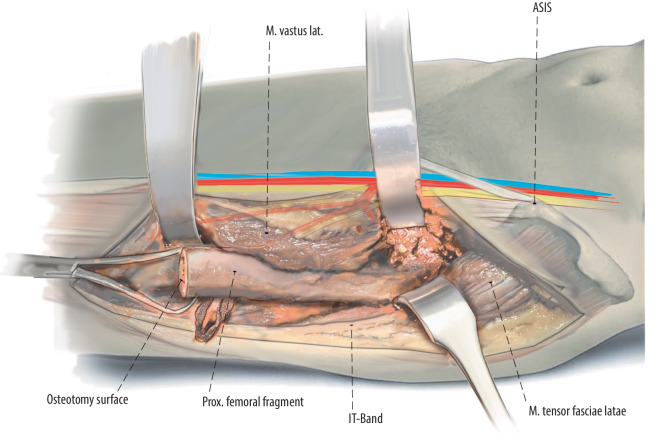
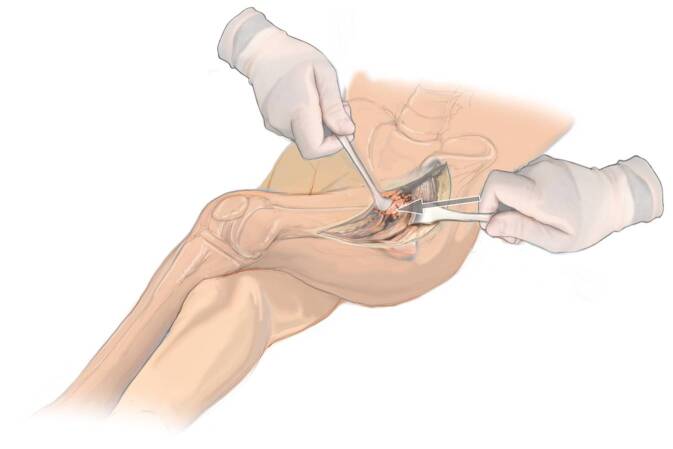
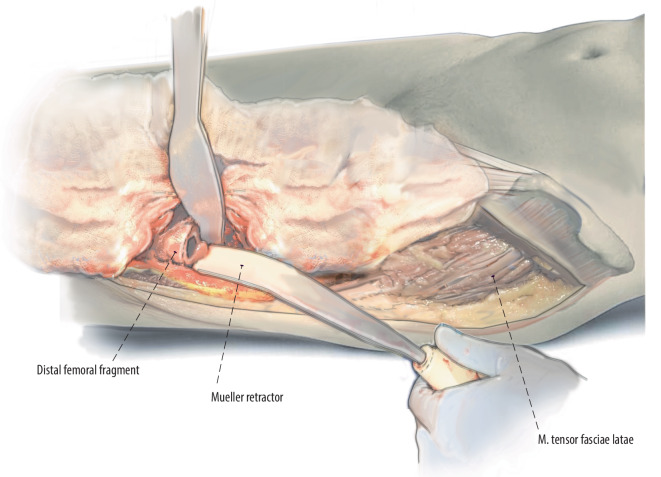
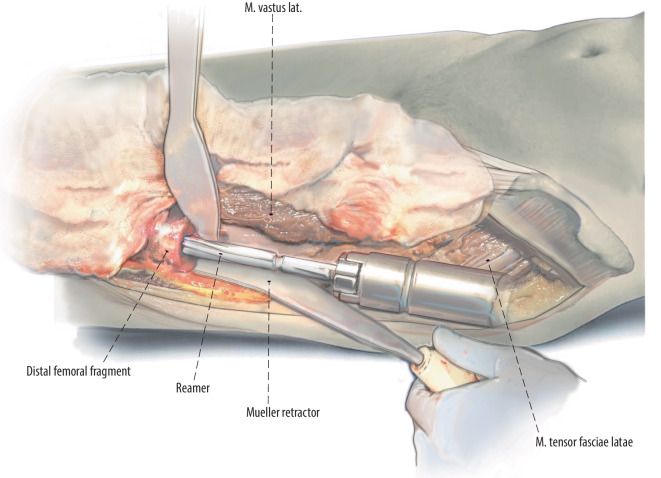
In contrast to conventional DAA approaches and extensions, we recommend starting the approach 3 cm lateral to the anterior superior iliac spine and performing a straight incision directed towards the fibular head. After identification and incision of the tensor fasciae lata proximally and the lateral mobilization of the iliotibial tract distally, the vastus lateralis muscle can be retracted medially as far as needed. Special care should be taken to avoid injuries to the branches of the femoral nerve innervating the vastus lateralis muscle. If required, the distal extension of the DAA can continue all the way to the knee to allow implantation of a total femoral replacement. The level of the femoral resection is detected with an x‑ray. In accordance with preoperative planning, the proximal femur is resected. Ream and broach the distal femoral fragment to the femoral canal. With trial implants in place, leg length, anteversion of the implant and hip stability are evaluated. It is crucial to provide robust reattachment of the abductor muscles to the PFR prosthesis. Mesh reinforcement can be used to reinforce the muscular attachment if necessary.
We typically use no hip precautions other than to limit combined external rotation and extension for 6 weeks. In most cases, full weight bearing is possible after surgery.
A PFR was performed in 16 patients (mean age: 55.1 years; range 17-84 years) using an extension of the DAA. The indication was primary bone sarcoma in 7 patients, metastatic lesion in 6 patients and massive periprosthetic femoral bone loss in 3 patients. Complications related to the surgery occurred in 2 patients (both were dislocation). Overall, 1 patient required reoperation and 1 patient died because of his disease. Mean follow-up was 34.5 months.
股骨近端置换术(PFR)是一种最初为肉瘤和转移性癌症切除后重建而开发的挽救性手术。这些技术也可以适应于涉及大量股骨近端骨丢失的非肿瘤性重建。直接前入路(DAA)易于用于翻修全髋关节置换术(THA),但很少有关于其用于股骨近端置换的报道。
无菌性、感染性股骨植入物松动、假体周围股骨骨折、股骨近端肿瘤病变。非肿瘤性股骨近端放置的最常见适应证是严重的股骨缺陷(Paprosky IIIB 或 IV)。
感染。
与传统的 DAA 入路和延长入路相比,我们建议在髂前上棘外侧 3cm 处开始入路,并向腓骨头方向做一条直线切口。在近端识别和切开阔筋膜张肌并向远端外侧移动阔筋膜张肌束后,可以根据需要将股外侧肌向内侧牵开。特别注意避免损伤支配股外侧肌的股神经分支。如果需要,DAA 的远端延长可以一直延伸到膝关节,以允许植入全股骨假体。股骨切除的水平通过 X 射线检测。根据术前规划,切除股骨近端。扩髓和扩孔股骨远端至股骨髓腔。安装试模后,评估下肢长度、植入物的前倾角和髋关节稳定性。为了提供强有力的外展肌附着于 PFR 假体非常重要。如果需要,可以使用网片加强来加强肌肉附着。
我们通常不采取任何髋关节预防措施,除了限制 6 周内联合外旋和伸展。在大多数情况下,手术后可以完全负重。
16 例患者(平均年龄:55.1 岁;范围 17-84 岁)采用 DAA 延长术行 PFR。7 例患者的适应证为原发性骨肉瘤,6 例为转移性病变,3 例为假体周围股骨骨量大量丢失。2 例患者发生与手术相关的并发症(均为脱位)。总的来说,1 例患者需要再次手术,1 例患者因疾病死亡。平均随访 34.5 个月。