Wellbeing and Preventable Chronic Diseases Division, Menzies School of Health Research, Charles Darwin University, Darwin, Northern Territory, Australia.
Department of Paediatrics, Division of Women, Children and Youth, Royal Darwin Hospital, Darwin, Northern Territory, Australia.
Pediatr Obes. 2022 Oct;17(10):e12932. doi: 10.1111/ijpo.12932. Epub 2022 May 29.
Few studies have assessed whether children exposed to in utero hyperglycaemia experience different growth trajectories compared to unexposed children.
To assess association of type 2 diabetes (T2D) and gestational diabetes mellitus (GDM) with early childhood weight, length/height and body mass index (BMI) trajectories, and with timing and magnitude of peak BMI in infancy.
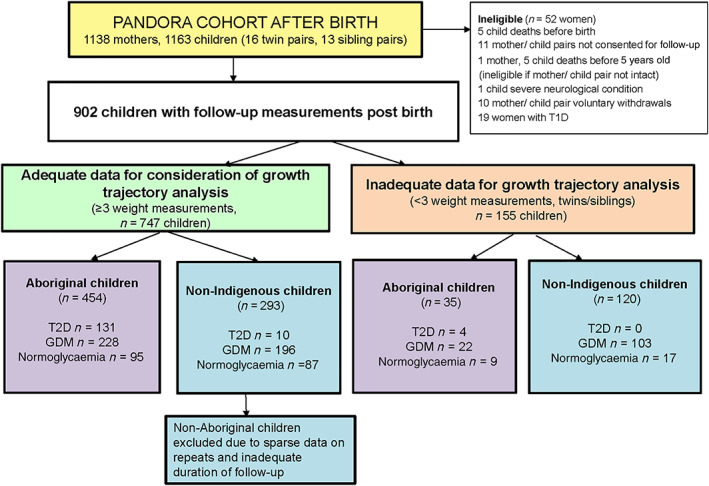
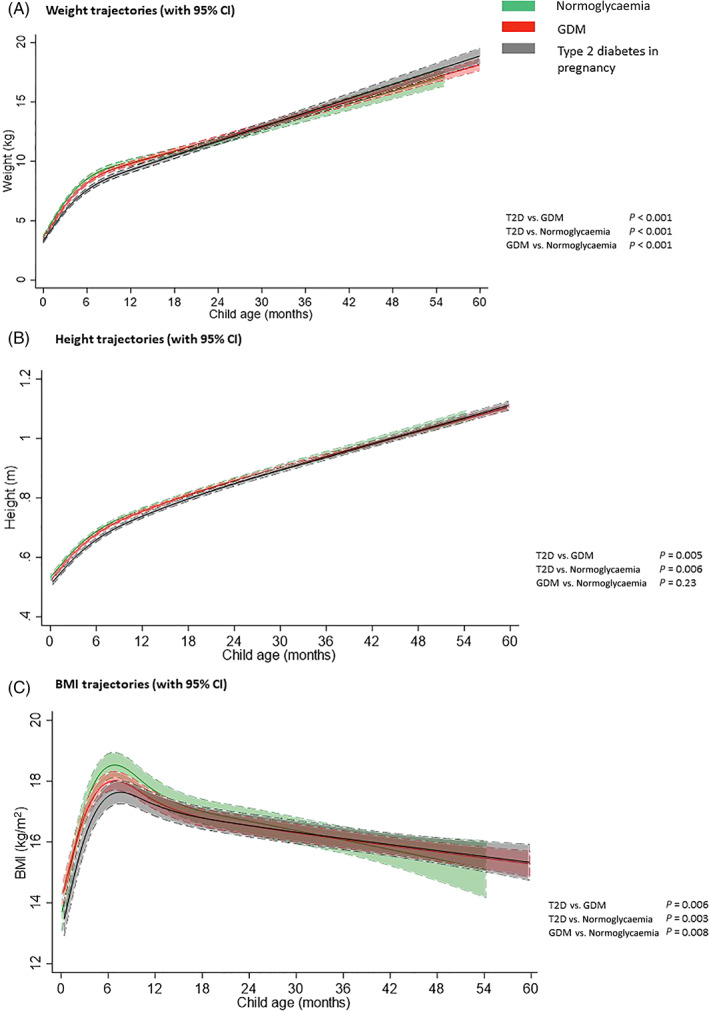
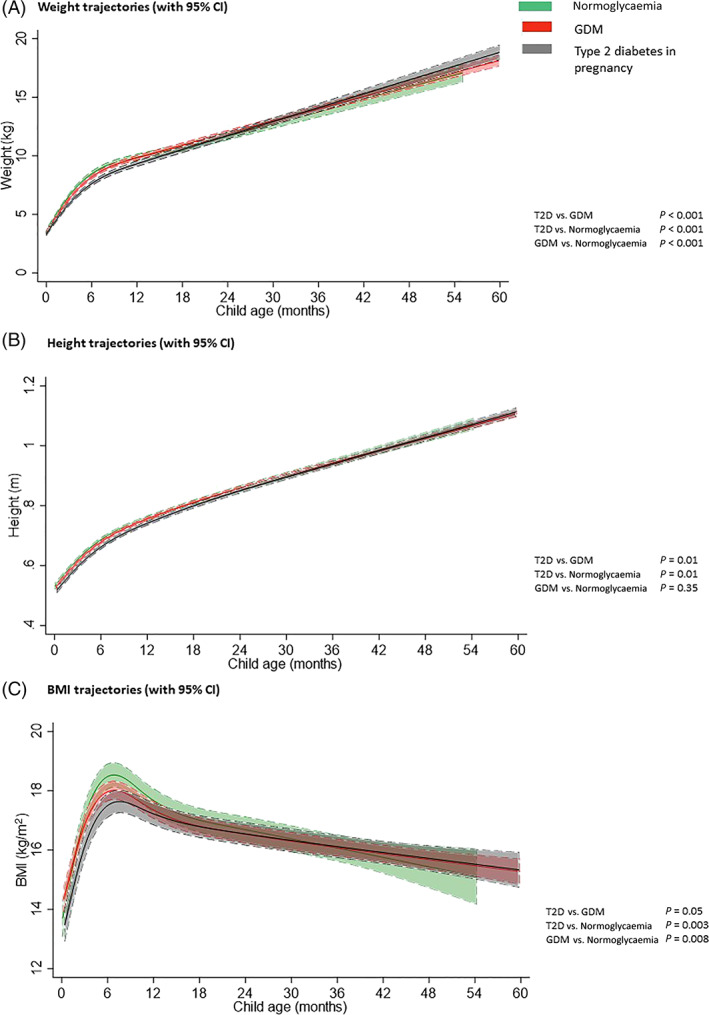
PANDORA is a birth cohort recruited from an Australian hyperglycaemia in pregnancy register, and women with normoglycaemia recruited from the community. Offspring growth measures were obtained from health records over a median follow-up of 3.0 years (interquartile range 1.9-4.0). This analysis included children born to Aboriginal mothers with in utero normoglycaemia (n = 95), GDM (n = 228) or T2D (n = 131). Growth trajectories (weight, length/height and BMI) were estimated using linear mixed models with cubic spline functions of child age.
After adjustment for maternal factors (age, BMI, parity, smoking, and socioeconomic measures) and child factors (age, gestational age at birth, and sex), children born to mothers with T2D or GDM had lower weight, length/height and BMI trajectories in infancy than children born to mothers with normoglycaemia, but similar weight and BMI by completion of follow-up. Children exposed to T2D had lower mean peak BMI 17.6 kg/m (95% confidence interval [CI] 17.3-18.0) than children exposed to normoglycaemia (18.6 kg/m [18.1-18.9]) (p = 0.001).
Maternal hyperglycaemia was associated with differences in early childhood growth trajectories after adjustment for maternal BMI. Exploration of associations between in utero hyperglycaemia exposure and growth trajectories into later childhood is required.
很少有研究评估宫内高血糖暴露的儿童与未暴露的儿童相比是否经历不同的生长轨迹。
评估 2 型糖尿病 (T2D) 和妊娠期糖尿病 (GDM) 与婴幼儿体重、身高/长度和体重指数 (BMI) 轨迹的关系,以及与婴儿期 BMI 峰值的时间和幅度的关系。
PANDORA 是从澳大利亚高血糖妊娠登记处招募的一个出生队列,以及从社区招募的血糖正常的女性。通过中位数随访 3.0 年(四分位间距 1.9-4.0 年)从健康记录中获取后代生长指标。本分析包括宫内血糖正常(n=95)、GDM(n=228)或 T2D(n=131)的土著母亲所生的儿童。使用线性混合模型和儿童年龄的三次样条函数来估计生长轨迹(体重、身高/长度和 BMI)。
在校正了母亲因素(年龄、BMI、产次、吸烟和社会经济措施)和儿童因素(年龄、出生时的胎龄和性别)后,与血糖正常的母亲所生的儿童相比,患有 T2D 或 GDM 的母亲所生的儿童在婴儿期的体重、身高/长度和 BMI 轨迹较低,但在随访结束时的体重和 BMI 相似。暴露于 T2D 的儿童的平均峰值 BMI 为 17.6kg/m(95%置信区间 [CI] 17.3-18.0),低于暴露于正常血糖的儿童(18.6kg/m [18.1-18.9])(p=0.001)。
校正母亲 BMI 后,母亲高血糖与婴幼儿生长轨迹的差异相关。需要探索宫内高血糖暴露与生长轨迹之间的关系,直至儿童后期。