Lie Ingrid Anne, Kaçar Sezgi, Wesnes Kristin, Brouwer Iman, Kvistad Silje S, Wergeland Stig, Holmøy Trygve, Midgard Rune, Bru Alla, Edland Astrid, Eikeland Randi, Gosal Sonia, Harbo Hanne F, Kleveland Grethe, Sørenes Yvonne S, Øksendal Nina, Varhaug Kristin N, Vedeler Christian A, Barkhof Frederik, Teunissen Charlotte E, Bø Lars, Torkildsen Øivind, Myhr Kjell-Morten, Vrenken Hugo
Department of Clinical Medicine, University of Bergen, Bergen, Norway
Neuro-SysMed, Department of Neurology, Haukeland University Hospital, Bergen, Norway.
J Neurol Neurosurg Psychiatry. 2022 Jun 1;93(8):849-57. doi: 10.1136/jnnp-2021-328568.
The predictive value of serum neurofilament light chain (sNfL) on long-term prognosis in multiple sclerosis (MS) is still unclear.
Investigate the relation between sNfL levels over a 2-year period in patients with relapsing-remitting MS, and clinical disability and grey matter (GM) atrophy after 10 years.
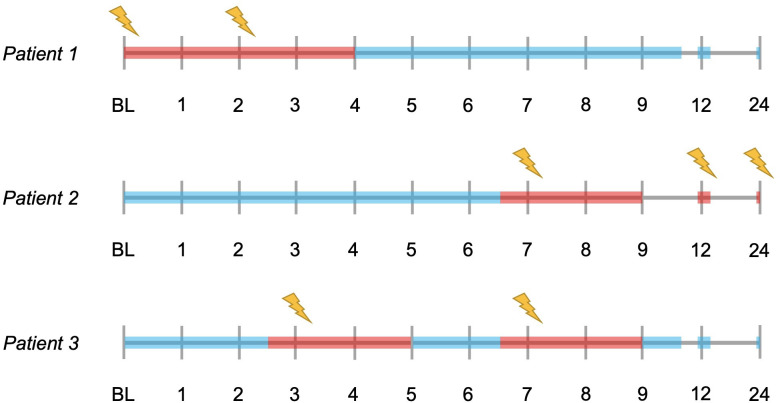
85 patients, originally enrolled in a multicentre, randomised trial of ω-3 fatty acids, participated in a 10-year follow-up visit. sNfL levels were measured by Simoa quarterly until month 12, and then at month 24. The appearance of new gadolinium-enhancing (Gd+) lesions was assessed monthly between baseline and month 9, and then at months 12 and 24. At the 10-year follow-up visit, brain atrophy measures were obtained using FreeSurfer.
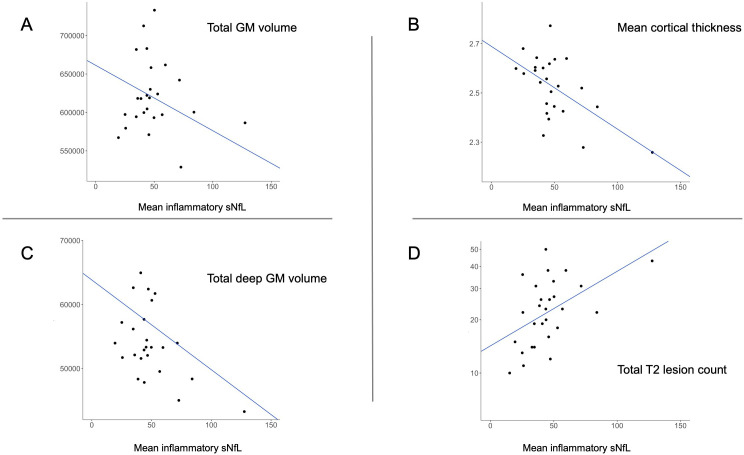
Higher mean sNfL levels during early periods of active inflammation (Gd+ lesions present or recently present) predicted lower total (β=-0.399, p=0.040) and deep (β=-0.556, p=0.010) GM volume, lower mean cortical thickness (β=-0.581, p=0.010) and higher T2 lesion count (β=0.498, p=0.018). Of the clinical outcomes, higher inflammatory sNfL levels were associated with higher disability measured by the dominant hand Nine-Hole Peg Test (β=0.593, p=0.004). Mean sNfL levels during periods of remission (no Gd+ lesions present or recently present) did not predict GM atrophy or disability progression.
Higher sNfL levels during periods of active inflammation predicted more GM atrophy and specific aspects of clinical disability 10 years later. The findings suggest that subsequent long-term GM atrophy is mainly due to neuroaxonal degradation within new lesions.
血清神经丝轻链(sNfL)对多发性硬化症(MS)长期预后的预测价值仍不明确。
研究复发缓解型MS患者2年内sNfL水平与10年后临床残疾及灰质(GM)萎缩之间的关系。
85名最初参加ω-3脂肪酸多中心随机试验的患者参与了为期10年的随访。sNfL水平通过Simoa每季度测量一次,直至第12个月,然后在第24个月测量。在基线至第9个月期间每月评估新钆增强(Gd+)病灶的出现情况,然后在第12个月和第24个月评估。在10年随访时,使用FreeSurfer获得脑萎缩测量值。
在炎症活动早期(存在或最近存在Gd+病灶)较高的平均sNfL水平预示着较低的总GM体积(β=-0.399,p=0.040)和深部GM体积(β=-0.556,p=0.010)、较低的平均皮质厚度(β=-0.581,p=0.010)以及较高的T2病灶计数(β=0.498,p=0.018)。在临床结局方面,较高的炎症性sNfL水平与优势手九孔插钉试验测量的较高残疾程度相关(β=0.593,p=0.004)。缓解期(不存在或最近不存在Gd+病灶)的平均sNfL水平不能预测GM萎缩或残疾进展。
炎症活动期较高的sNfL水平预示着10年后更多的GM萎缩和临床残疾的特定方面。研究结果表明,随后的长期GM萎缩主要是由于新病灶内的神经轴突退化。