Alzheimer Center Erasmus MC, Department of Neurology, Erasmus University Medical Center, Rotterdam, The Netherlands.
Alzheimer Center Amsterdam, Neurology, Vrije Universiteit Amsterdam, Amsterdam UMC location VUmc, Amsterdam, The Netherlands.
Alzheimers Res Ther. 2022 Jun 1;14(1):77. doi: 10.1186/s13195-022-01018-3.
Many families with clinical early-onset Alzheimer's disease (EOAD) remain genetically unexplained. A combination of genetic factors is not standardly investigated. In addition to monogenic causes, we evaluated the possible polygenic architecture in a large series of families, to assess if genetic testing of familial EOAD could be expanded.
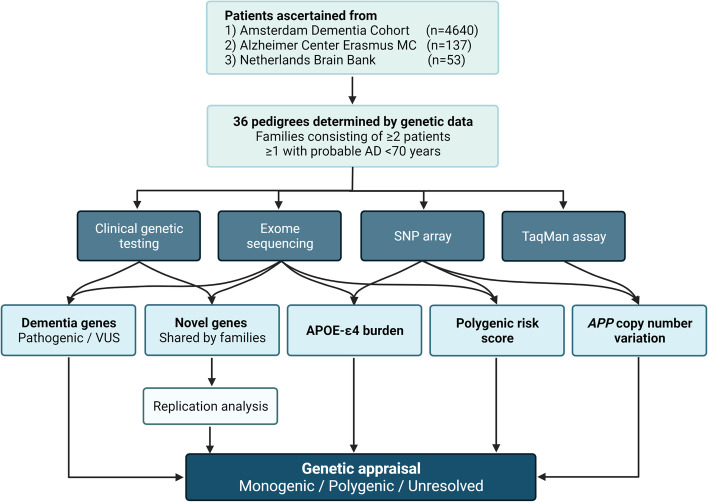
Thirty-six pedigrees (77 patients) were ascertained from a larger cohort of patients, with relationships determined by genetic data (exome sequencing data and/or SNP arrays). All families included at least one AD patient with symptom onset <70 years. We evaluated segregating rare variants in known dementia-related genes, and other genes or variants if shared by multiple families. APOE was genotyped and duplications in APP were assessed by targeted test or using SNP array data. We computed polygenic risk scores (PRS) compared with a reference population-based dataset, by imputing SNP arrays or exome sequencing data.
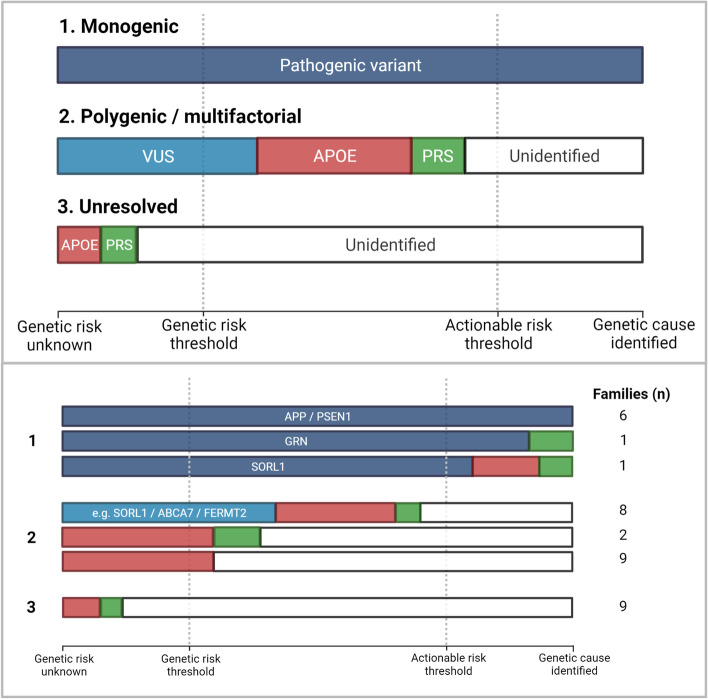
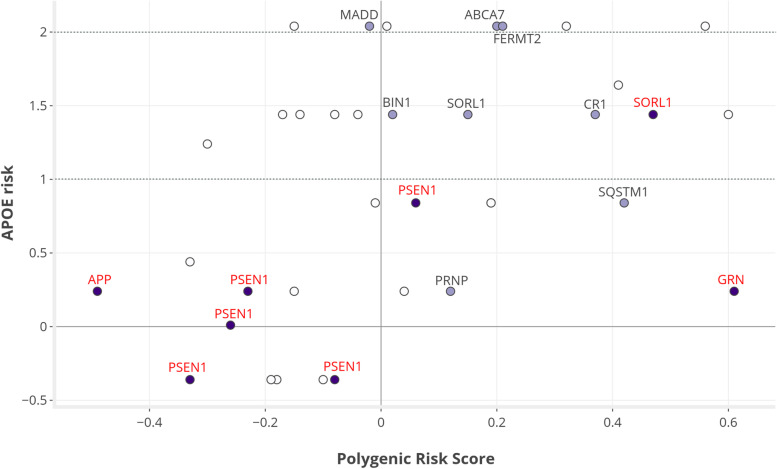
In eight families, we identified a pathogenic variant, including the genes APP, PSEN1, SORL1, and an unexpected GRN frameshift variant. APOE-ε4 homozygosity was present in eighteen families, showing full segregation with disease in seven families. Eight families harbored a variant of uncertain significance (VUS), of which six included APOE-ε4 homozygous carriers. PRS was not higher in the families combined compared with the population mean (beta 0.05, P = 0.21), with a maximum increase of 0.61 (OR = 1.84) in the GRN family. Subgroup analyses indicated lower PRS in six APP/PSEN1 families compared with the rest (beta -0.22 vs. 0.10; P = 0.009) and lower APOE burden in all eight families with monogenic cause (beta 0.29 vs. 1.15, P = 0.010). Nine families remained without a genetic cause or risk factor identified.
Besides monogenic causes, we suspect a polygenic disease architecture in multiple families based on APOE and rare VUS. The risk conveyed by PRS is modest across the studied families. Families without any identified risk factor render suitable candidates for further in-depth genetic evaluation.
许多有临床早发性阿尔茨海默病(EOAD)家族的遗传背景仍未得到解释。遗传因素的组合并未得到标准研究。除了单基因病因外,我们还在一个大型家族系列中评估了可能的多基因结构,以评估是否可以扩大对家族性 EOAD 的基因检测。
从更大的患者队列中确定了 36 个家系(77 例患者),通过遗传数据(外显子组测序数据和/或 SNP 数组)确定关系。所有家系均至少包括一名症状发作<70 岁的 AD 患者。我们评估了已知与痴呆相关的基因中分离的罕见变异,以及如果多个家系共享的其他基因或变异。通过基因分型 APOE,通过靶向测试或使用 SNP 数组数据评估 APP 中的重复。我们计算了与基于参考人群的数据集相比的多基因风险评分(PRS),通过外显子组测序数据或 SNP 数组数据进行了估算。
在 8 个家系中,我们发现了致病性变异,包括 APP、PSEN1、SORL1 基因和一个意想不到的 GRN 移码变异。18 个家系中存在 APOE-ε4 纯合子,其中 7 个家系中疾病完全与 APOE-ε4 纯合子分离。8 个家系携带有不确定意义的变异(VUS),其中 6 个包括 APOE-ε4 纯合子携带者。与人群平均值相比,合并家系的 PRS 没有更高(β 0.05,P = 0.21),在 GRN 家系中最大增加了 0.61(OR = 1.84)。亚组分析表明,与其余家系相比,六个 APP/PSEN1 家系的 PRS 较低(β -0.22 与 0.10;P = 0.009),并且所有 8 个具有单基因病因的家系中的 APOE 负担较低(β 0.29 与 1.15,P = 0.010)。九个家系仍然没有发现遗传原因或风险因素。
除了单基因病因外,我们还怀疑多个家系存在 APOE 和罕见 VUS 的多基因疾病结构。研究家系的 PRS 所带来的风险适中。没有任何确定风险因素的家系适合进一步进行深入的遗传评估。