Chinese PLA Medical School, Beijing, China.
Senior Department of Hepatology, the Fifth Medical Center of PLA General Hospital, Beijing, China.
Front Immunol. 2022 May 16;13:885829. doi: 10.3389/fimmu.2022.885829. eCollection 2022.
Acute-on-chronic liver failure (ACLF) has a high mortality rate. The role of granulocyte colony-stimulating factor (G-CSF) in ACLF remains controversial. Monocytes/macrophages are core immune cells, which are involved in the initiation and progression of liver failure; however, the effect of G-CSF on monocytes/macrophages is unclear. The study aimed to verify the clinical efficacy of G-CSF and explore the effect of it on monocytes in hepatitis B virus (HBV)-related ACLF (HBV-ACLF) paitents.
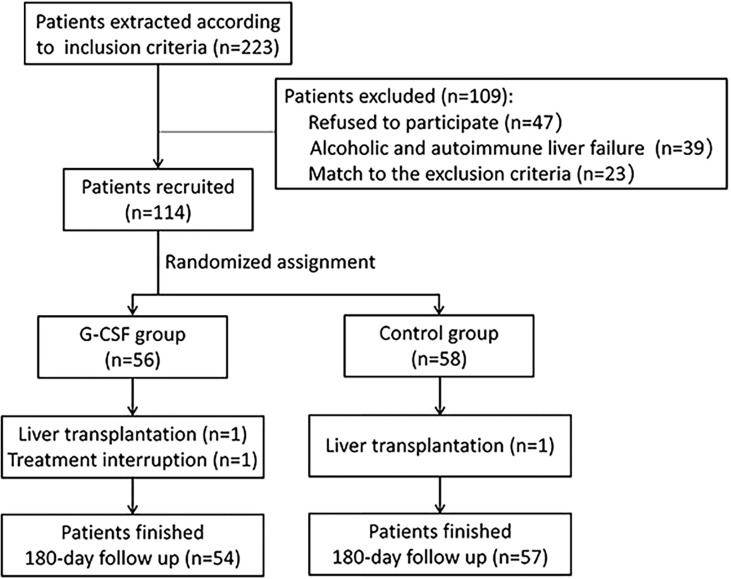
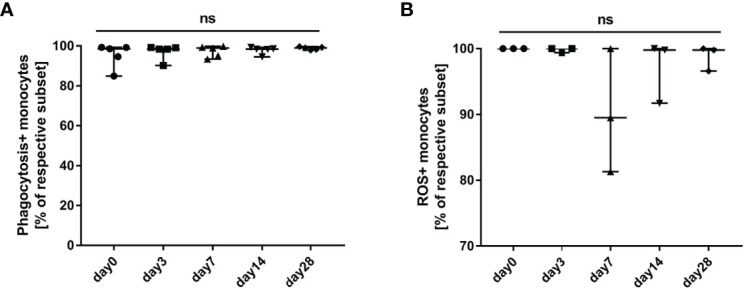
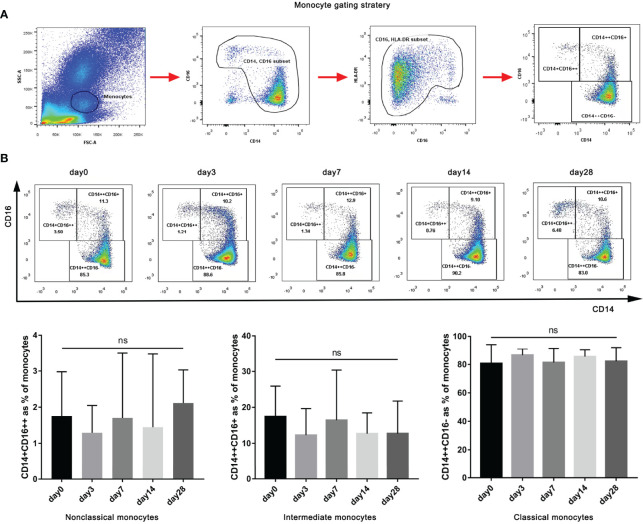
We performed a large randomized controlled clinical trial for the treatment of HBV-ACLF using G-CSF. A total of 111 patients with HBV-ACLF were prospectively randomized into the G-CSF group (5 μg/kg G-CSF every day for 6 days, then every other day until day 18) or the control group (standard therapy). All participants were followed up for at least 180 days. The relationship between monocyte count and mortality risk was analyzed. The effect of G-CSF on the phenotype and function of monocytes from patients with HBV-ACLF was evaluated using flow cytometry and experiments.
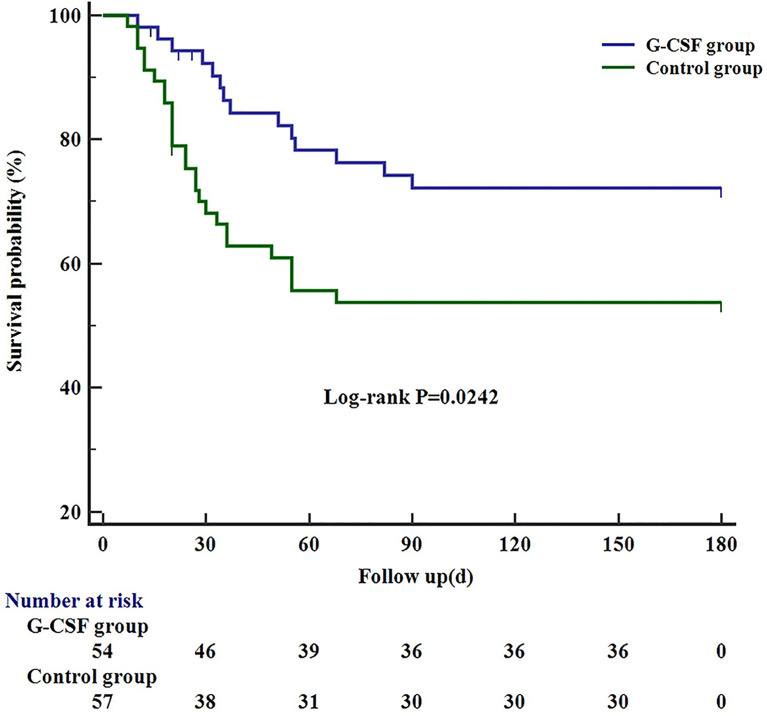
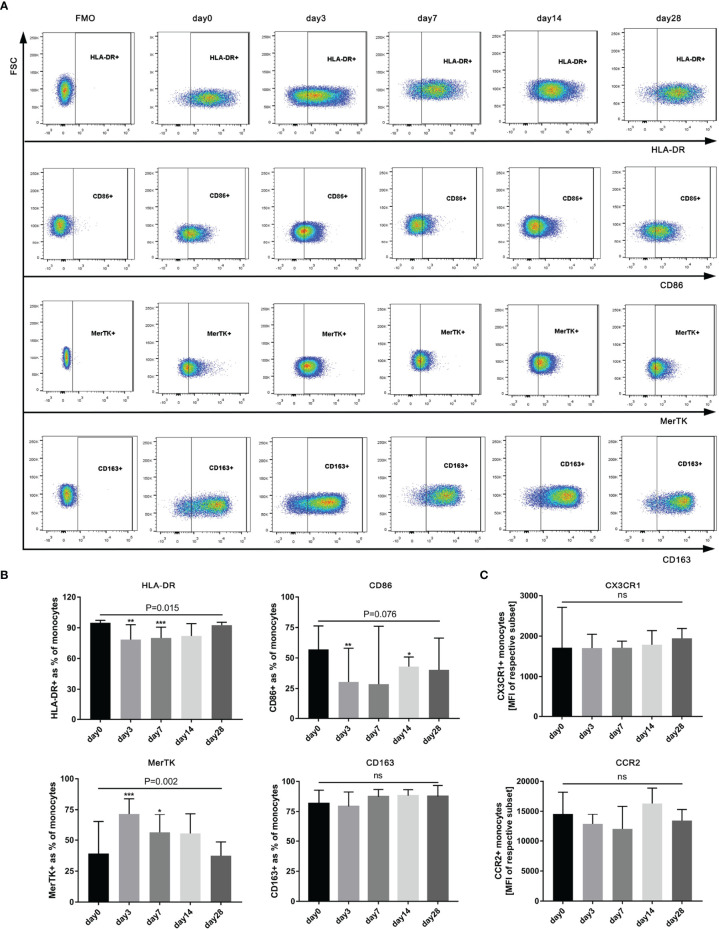
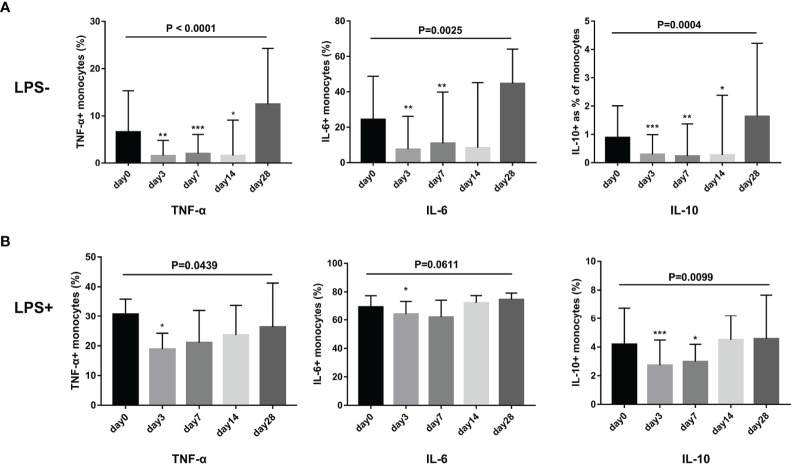
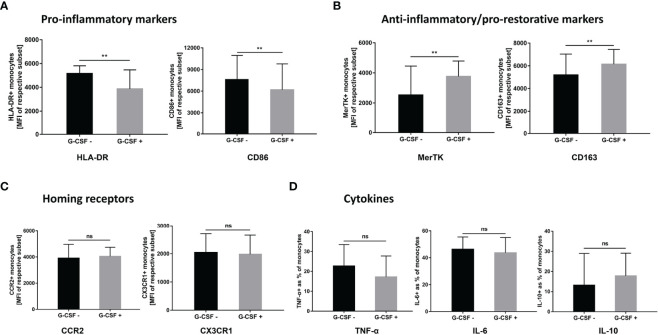
The survival probability of the G-CSF group at 180 days was higher than that of the control group (72.2% vs. 53.8%, = 0.0142). In the G-CSF-treated group, the monocyte counts on days 0 and 7 were independently associated with an evaluated mortality risk in the fully adjusted model (Model 3) [at day 0: hazard ratio (HR) 95% confidence interval (CI): 15.48 (3.60, 66.66), = 0.0002; at day 7: HR (95% CI): 1.10 (0.50, 2.43), =0.8080]. Further analysis showed that after treatment with G-CSF in HBV-ACLF patients, the expression of M1-like markers (HLA-DR and CD86) in monocytes decreased (HLA-DR: = 0.0148; CD86: = 0.0764). The expression of MerTK (M2-like marker) increased ( = 0.0002). The secretion of TNF-α, IL-6, and IL-10 from monocytes decreased without lipopolysaccharide (LPS) stimulation (TNF-α: < 0.0001; IL-6: = 0.0025; IL-10: = 0.0004) or with LPS stimulation (TNF-α: = 0.0439; = 0.0611; IL-10: = 0.0099). Similar effects were observed experiments.
G-CSF therapy confers a survival benefit to patients with HBV-ACLF. G-CSF can promote the anti-inflammatory/pro-restorative phenotype (M2-like) transition of monocytes, which may contribute to the recovery of ACLF. ClinicalTrials.gov, identifier (NCT02331745).
慢加急性肝衰竭(ACLF)的死亡率较高。粒细胞集落刺激因子(G-CSF)在 ACLF 中的作用仍存在争议。单核细胞/巨噬细胞是核心免疫细胞,参与肝衰竭的启动和进展;然而,G-CSF 对单核细胞/巨噬细胞的影响尚不清楚。本研究旨在验证 G-CSF 的临床疗效,并探讨其对乙型肝炎病毒(HBV)相关 ACLF(HBV-ACLF)患者单核细胞的影响。
我们进行了一项使用 G-CSF 治疗 HBV-ACLF 的大型随机对照临床试验。前瞻性随机将 111 例 HBV-ACLF 患者分为 G-CSF 组(每天 5μg/kg G-CSF,连用 6 天,然后每两天一次至第 18 天)或对照组(标准治疗)。所有参与者均至少随访 180 天。分析单核细胞计数与死亡率风险的关系。使用流式细胞术和实验评估 G-CSF 对 HBV-ACLF 患者单核细胞表型和功能的影响。
180 天时 G-CSF 组的生存率高于对照组(72.2%比 53.8%, = 0.0142)。在 G-CSF 治疗组中,第 0 天和第 7 天的单核细胞计数与完全调整模型(模型 3)中的评估死亡率风险独立相关[第 0 天:危险比(HR)95%置信区间(CI):15.48(3.60,66.66), = 0.0002;第 7 天:HR(95%CI):1.10(0.50,2.43), = 0.8080]。进一步分析表明,在 HBV-ACLF 患者中使用 G-CSF 治疗后,单核细胞中 M1 样标志物(HLA-DR 和 CD86)的表达降低(HLA-DR: = 0.0148;CD86: = 0.0764)。MerTK(M2 样标志物)的表达增加( = 0.0002)。单核细胞在没有脂多糖(LPS)刺激(TNF-α: < 0.0001;IL-6: = 0.0025;IL-10: = 0.0004)或 LPS 刺激(TNF-α: = 0.0439; = 0.0611;IL-10: = 0.0099)时的 TNF-α、IL-6 和 IL-10 分泌减少。实验中观察到类似的效果。
G-CSF 治疗可使 HBV-ACLF 患者获得生存获益。G-CSF 可促进单核细胞抗炎/修复表型(M2 样)的转化,这可能有助于 ACLF 的恢复。ClinicalTrials.gov,标识符(NCT02331745)。