Division of Integrative Systems Medicine and Digestive Disease, Imperial College London, London, United Kingdom.
Division of Immunology and Inflammation, Imperial College London, London, United Kingdom.
Front Immunol. 2018 Dec 14;9:2948. doi: 10.3389/fimmu.2018.02948. eCollection 2018.
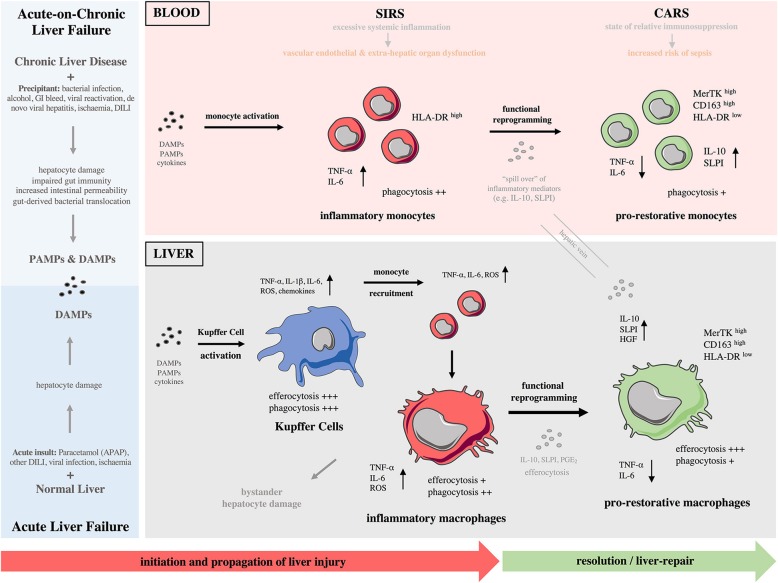
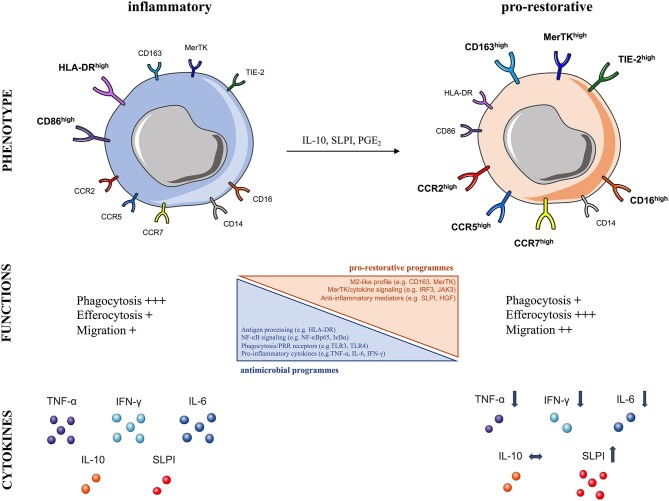
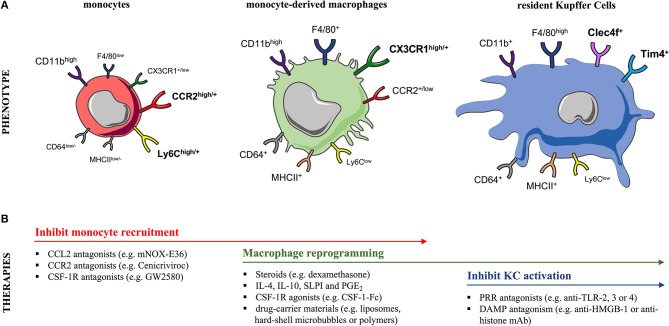
Acute and acute-on-chronic liver failure (ALF and ACLF), though distinct clinical entities, are considered syndromes of innate immune dysfunction. Patients with ALF and ACLF display evidence of a pro-inflammatory state with local liver inflammation, features of systemic inflammatory response syndrome (SIRS) and vascular endothelial dysfunction that drive progression to multi-organ failure. In an apparent paradox, these patients are concurrently immunosuppressed, exhibiting acquired immune defects that render them highly susceptible to infections. This paradigm of tissue injury succeeded by immunosuppression is seen in other inflammatory conditions such as sepsis, which share poor outcomes and infective complications that account for high morbidity and mortality. Monocyte and macrophage dysfunction are central to disease progression of ALF and ACLF. Activation of liver-resident macrophages (Kupffer cells) by pathogen and damage associated molecular patterns leads to the recruitment of innate effector cells to the injured liver. Early monocyte infiltration may contribute to local tissue destruction during the propagation phase and results in secretion of pro-inflammatory cytokines that drive SIRS. In the hepatic microenvironment, recruited monocytes mature into macrophages following local reprogramming so as to promote resolution responses in a drive to maintain tissue integrity. Intra-hepatic events may affect circulating monocytes through spill over of soluble mediators and exposure to apoptotic cell debris during passage through the liver. Hence, peripheral monocytes show numerous acquired defects in acute liver failure syndromes that impair their anti-microbial programmes and contribute to enhanced susceptibility to sepsis. This review will highlight the cellular and molecular mechanisms by which monocytes and macrophages contribute to the pathophysiology of ALF and ACLF, considering both hepatic inflammation and systemic immunosuppression. We identify areas for further research and potential targets for immune-based therapies to treat these devastating conditions.
急性肝衰竭(ALF)和慢加急性肝衰竭(ACLF),尽管是两种不同的临床实体,但被认为是固有免疫功能障碍的综合征。ALF 和 ACLF 患者表现出局部肝脏炎症的促炎状态、全身炎症反应综合征(SIRS)和血管内皮功能障碍的特征,这些特征导致多器官衰竭的进展。显然存在矛盾的是,这些患者同时存在免疫抑制,表现出获得性免疫缺陷,使他们极易感染。这种组织损伤继之以免疫抑制的范例可见于其他炎症性疾病,如败血症,它们的预后较差,感染并发症发生率高,导致高发病率和死亡率。单核细胞和巨噬细胞功能障碍是 ALF 和 ACLF 疾病进展的核心。病原体和损伤相关分子模式激活肝固有巨噬细胞(库普弗细胞),导致固有效应细胞募集到受损的肝脏。早期单核细胞浸润可能导致传播阶段的局部组织破坏,并导致促炎细胞因子的分泌,从而驱动 SIRS。在肝微环境中,募集的单核细胞在局部重编程后成熟为巨噬细胞,以促进组织完整性的维持反应。肝内事件可能通过可溶性介质的溢出和通过肝脏传递时暴露于凋亡细胞碎片来影响循环单核细胞。因此,外周单核细胞在急性肝衰竭综合征中表现出许多获得性缺陷,损害其抗微生物程序,并导致对败血症的易感性增强。本综述将重点介绍单核细胞和巨噬细胞在 ALF 和 ACLF 病理生理学中的细胞和分子机制,同时考虑肝内炎症和全身免疫抑制。我们确定了进一步研究的领域和潜在的免疫治疗靶点,以治疗这些破坏性疾病。