Centre for Applied Pharmacokinetic Research, Division of Pharmacy and Optometry, School of Health Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK.
Development Planning, Clinical Development Center, Asahi Kasei Pharma Corporation, Tokyo, Japan.
Clin Pharmacol Ther. 2022 Sep;112(3):615-626. doi: 10.1002/cpt.2672. Epub 2022 Jun 28.
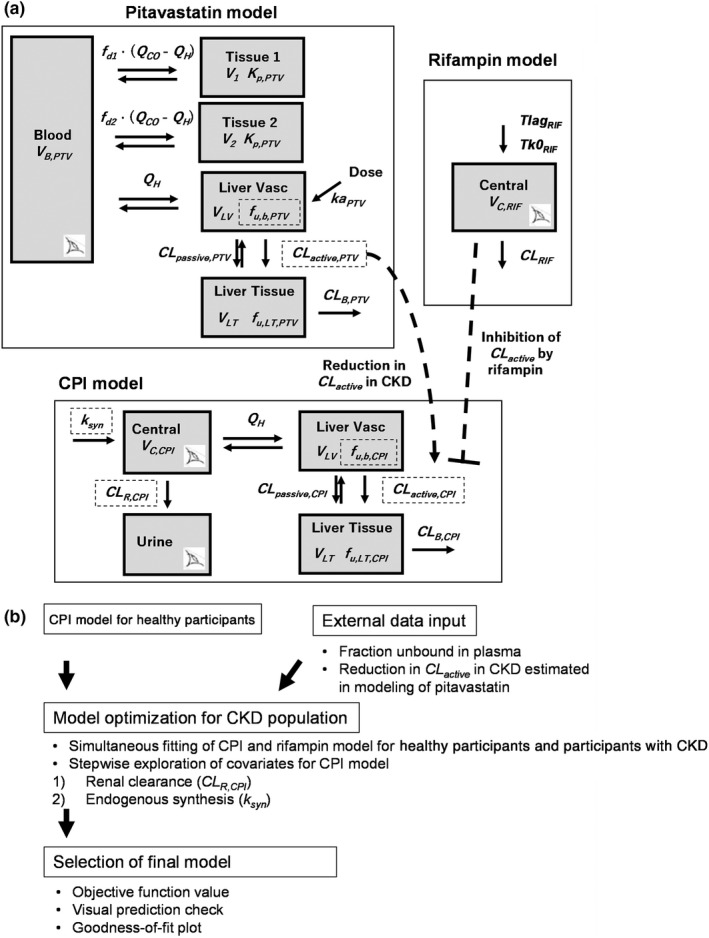
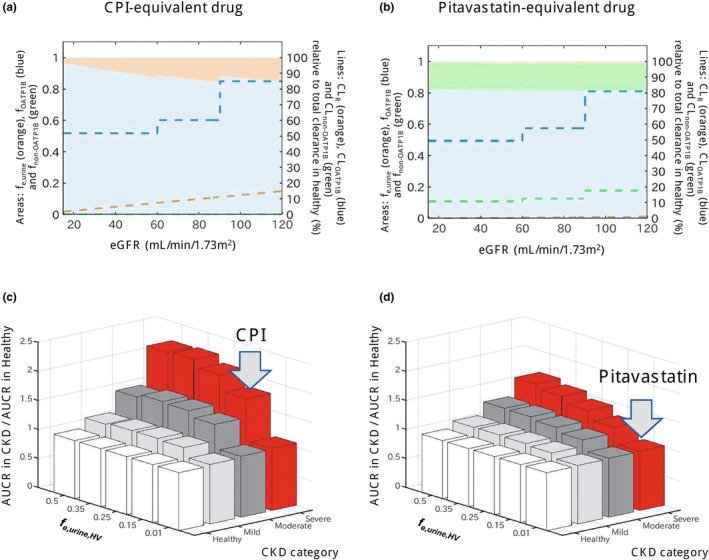
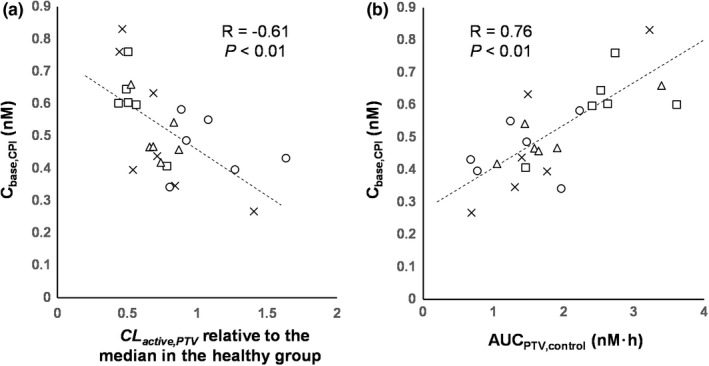
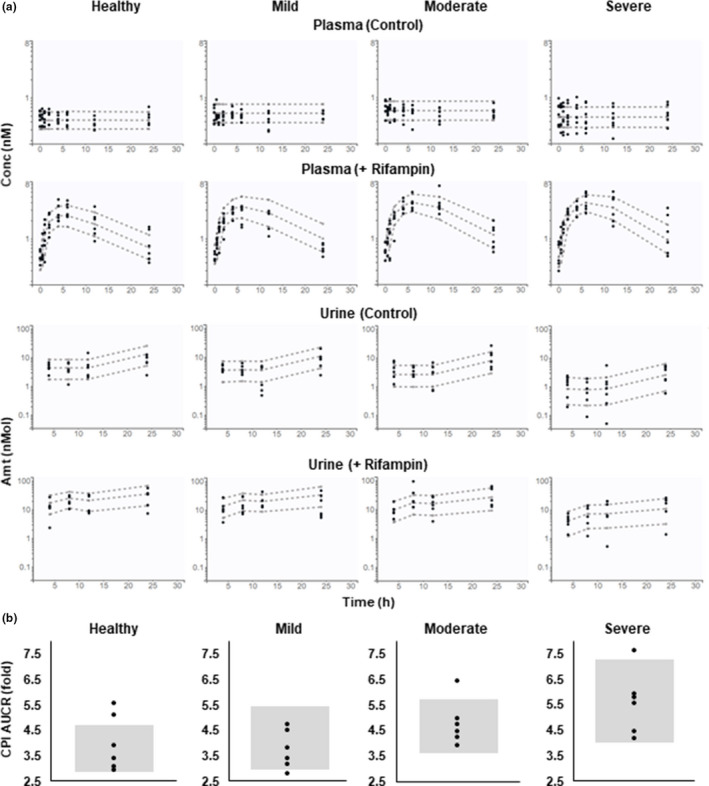
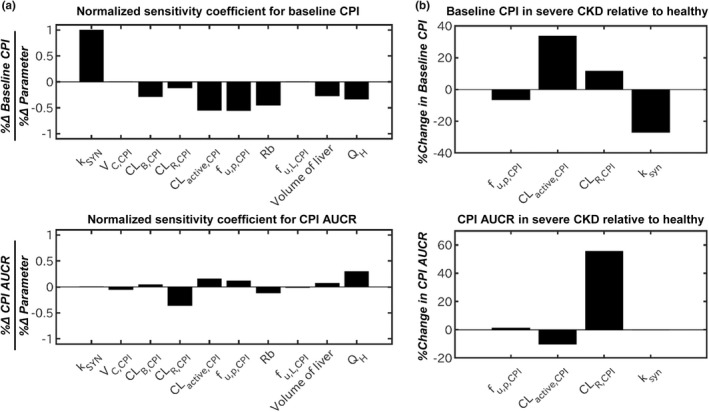
Coproporphyrin I (CPI) is an endogenous biomarker of organic anion transporting polypeptide 1B transporter (OATP1B). CPI plasma baseline was reported to increase with severity of chronic kidney disease (CKD). Further, ratio of CPI area under the plasma concentration-time curve (AUCR) in the presence/absence of OATP1B inhibitor rifampin was higher in patients with CKD compared with healthy participants, in contrast to pitavastatin (a clinical OATP1B probe). This study investigated mechanism(s) contributing to altered CPI baseline in patients with CKD by extending a previously developed physiologically-based pharmacokinetic (PBPK) model to this patient population. CKD-related covariates were evaluated in a stepwise manner on CPI fraction unbound in plasma (f ), OATP1B-mediated hepatic uptake clearance (CL ), renal clearance (CL ), and endogenous synthesis (k ). The CPI model successfully recovered increased baseline and rifampin-mediated AUCR in patients with CKD by accounting for the following disease-related changes: 13% increase in f , 29% and 39% decrease in CL in mild and moderate to severe CKD, respectively, decrease in CL proportional to decline in glomerular filtration rate, and 27% decrease in k in severe CKD. Almost complete decline in CPI renal elimination in severe CKD increased its fraction transported by OATP1B, rationalizing differences in the CPI-rifampin interaction observed between healthy participants and patients with CKD. In conclusion, mechanistic modeling performed here supports CKD-related decrease in OATP1B function to inform prospective PBPK modeling of OATP1B-mediated drug-drug interaction in these patients. Monitoring of CPI allows detection of CKD-drug interaction risk for OATP1B drugs with combined hepatic and renal elimination which may be underestimated by extrapolating the interaction risk based on pitavastatin data in healthy participants.
粪卟啉 I(CPI)是有机阴离子转运多肽 1B 转运体(OATP1B)的内源性生物标志物。有报道称,CPI 血浆基线随着慢性肾脏病(CKD)的严重程度而增加。此外,与匹伐他汀(一种临床 OATP1B 探针)相比,在 CKD 患者中,存在/不存在 OATP1B 抑制剂利福平时,CPI 血浆浓度-时间曲线下面积(AUCR)的比值更高。本研究通过将先前开发的基于生理学的药代动力学(PBPK)模型扩展到该患者人群,研究了导致 CKD 患者 CPI 基线改变的机制。以逐步的方式评估了与 CKD 相关的协变量对 CPI 血浆未结合分数(f)、OATP1B 介导的肝脏摄取清除率(CL)、肾脏清除率(CL)和内源性合成(k)的影响。CPI 模型通过考虑以下与疾病相关的变化成功地恢复了 CKD 患者的基线增加和利福平介导的 AUCR:f 增加 13%,轻度和中度至重度 CKD 患者的 CL 分别降低 29%和 39%,CL 与肾小球滤过率下降成比例降低,以及重度 CKD 患者的 k 降低 27%。严重 CKD 中 CPI 肾脏消除几乎完全下降,增加了其通过 OATP1B 的转运分数,合理解释了健康参与者和 CKD 患者之间观察到的 CPI-利福平相互作用的差异。总之,这里进行的机制建模支持与 CKD 相关的 OATP1B 功能下降,以告知这些患者中 OATP1B 介导的药物相互作用的前瞻性 PBPK 建模。监测 CPI 可以检测具有肝和肾消除的 OATP1B 药物的 CKD-药物相互作用风险,这可能会根据健康参与者的匹伐他汀数据外推相互作用风险而被低估。